دوره 6، شماره 2 - ( 6-1399 )
جلد 6 شماره 2 صفحات 85-66 |
برگشت به فهرست نسخه ها


![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Norasteh A A, Payandeh M, Mohammad Ashour Z. Investigation of Knee Arthrokinematic Changes Before and After Reconstruction of Anterior Cruciate Ligament: A Systematic Review. J Sport Biomech 2020; 6 (2) :66-85
URL: http://biomechanics.iauh.ac.ir/article-1-222-fa.html
URL: http://biomechanics.iauh.ac.ir/article-1-222-fa.html
نورسته علی اصغر، پاینده مصطفی، محمد عاشور زاهر. بررسی تغییرات آرتروکینماتیک زانو قبل و بعد از بازسازی رباط متقاطع قدامی: یک مطالعه مروری نظاممند. مجله بیومکانیک ورزشی. 1399; 6 (2) :66-85



1- گروه آسیب شناسی ورزشی و حرکات اصلاحی، دانشکده تربیتبدنی و علوم ورزشی، دانشگاه گیلان، رشت، ایران.
واژههای کلیدی: اختلالات حرکت، پارگی رباط متقاطع قدامی، رباط متقاطع قدامی بازسازی شده، استئوآرتریت زانو
متن کامل [PDF 9063 kb]
(1502 دریافت)
| چکیده (HTML) (3075 مشاهده)
متن کامل: (7620 مشاهده)
مقدمه
انجامشدن حرکات رول، گلاید و چرخش در مفصل زانو به شکل طبیعی، که نشاندهنده ثبات این مفصل است، به وسیله شکل کندیلها، منیسکها و ساختارهای حمایتکننده پاسیو که مهمترین آنها چهار رباط اصلی زانوست، فراهم میشود [1]. از بین ساختارهای اشارهشده رباط متقاطع قدامی نقش کلیدی را در ثبات زانو ایفا میکند [2]. آسیب این رباط در بین آسیبهای ورزشی یکی از رایجترین و ناتوانکنندهترین آسیبها محسوب میشود [3]. تحقیقات اخیر اشاره کردهاند که میزان شیوع آسیب رباط متقاطع قدامی در افراد زیر هفده سال، به خصوص در افراد بین ده تا چهارده سال، بهسرعت در حال افزایش است [4]. یکی از اولین و مهمترین پیامدهای این آسیب در مفصل احتمال بروز آرتروز در مفصل زانوست [5].
در هنگام فلکشن و اکستنشن در مفصل تیبیوفمورال ترکیبی از حرکات رول، گلاید (اسلاید) و چرخش در سطح مفصل اتفاق میافتد که برای حفظ تجانس دو استخوان ران و درشتنی روی همدیگر در هنگام حرکت ضروری است [6]. در مفصل زانو در هنگام حرکت، نسبت مقادیر رول و گلاید از طریق بررسی مسیر مرکز لحظهای چرخش استنباط میشود [7-10]. درواقع عملکرد اصلی رباط متقاطع قدامی ایجاد ثبات در حرکات انتقالی و چرخش تیبیا نسبت به فمور است [7، 10]. رباط متقاطع قدامی دارای دو باند قدامی داخلی و خلفی خارجی است. باند قدامی داخلی هنگامی که زانو به فلکشن میرود، سفت و محکم میشود و باند خلفی خارجی نیز در زمان اکستنشن زانو در حالت سفت و محکم قرار میگیرد. این ترتیب عملکرد در رباط متقاطع قدامی نشاندهنده اعمال نقش این رباط در سرتاسر دامنه حرکتی فلکشن و اکستنشن است [8].
همچنین رباط متقاطع قدامی، نگهدارنده اصلی جابهجایی قدامی تیبیا روی فمور در حرکت هایپر اکستنش و همچنین جلوگیریکننده از واروس و والگوس زانو در هنگام اکستنش کامل است. همچنین این رباط از چرخش داخلی و خارجی زانو نیز در هنگام اکستنشِ کامل جلوگیری میکند [11]. البته باید اشاره شود که با ابداع تکنولوژیهای پیشرفته، میزان این حرکات به میلیمتر به شکل بسیار دقیق اندازهگیری شده است که نتایج آنها به ما نشان میدهد درک آرتروکینماتیک مفصل تیبیوفمورال از آنچه تصور میشود، پیچیدهتر است. برای نمونه خاصیان و همکاران به وسیله فلورسکوپی به روش دوبُعدی و سهبُعدی، گزارش کردند که از اکستنش کامل تا حداکثر فلکشن زانو در خلف اپیکندیل خارجی ران به طور متوسط 2±2/5 میلیمتر رول خلفی و در اپیکندیل داخلی به مقدار 2/2 ± 2/5 میلیمتر رول قدامی ایجاد میشود [12].
مطالعات گذشته ثابت کردهاند که حتی رباط متقاطع قدامی آسیبدیده که بازسازی شده است، نشانههایی از بیثباتی را نشان میدهد [13-21]. با توجه به نقش محوری رباط متقاطع قدامی در کنترل ثبات و پایداری مفصل زانو [22]، ثابت شده است پارگی آن منجر به کاهش حس عمقی، تعادل، قدرت، عملکرد عضلانی و همانطور که اشاره شد، تغییرات بیومکانیکی خواهد شد [23]. همچنین در اثر آسیب این رباط الگوی بارهای واردشده بر سطوح مفصلی تغییر خواهد کرد. تغییر این الگو باعث ورود بارهای غیرطبیعی روی غضروف سطوح مفصلی در طی فعالیتهای عملکردی شده و درنهایت این تغییرات منجر به تخریب سطوح غضروف و بروز یا پیشرفت استئوآرتریت میشود [24، 25]. فهم دقیق تغییرات جزئی آرتروکینماتیکی حاصل از پارگی رباط متقاطع قدامی اینجا هم اهمیت پیدا میکند که طبق گزارش بارینیوس و همکاران حتی بعد از بازسازی رباط متقاطع قدامی نیز 57 درصد از افرادی که طی چهارده سال تحت نظر بودند، در زانوی آسیبدیده دچار پیشرفت استئوآرتریت شده بودند [26]. موارد اشارهشده این پرسش را ایجاد میکند که مگر بعد از پارگی رباط متقاطع قدامی و حتی بعد از بازسازی آن چه تغییرات آرتروکینماتیکی رخ میدهد که این تغییرات باعث عوارض برگشتناپذیر میشود؟ متأسفانه هیچ مقاله مروری داخلی و خارجیای نیافتیم که این سؤال را در قالب جامعتر و دقیقتری پاسخ دهد؛ بنابراین هدف از تحقیق مروری حاضر پی بردن به مهمترین تغییرات آرتروکینماتیکی بعد از پارگی رباط متقاطع قدامی (چه قبل و چه بعد از بازسازی و همچنین بعد از یک دوره توانبخشی) با توجه به تحقیقات گذشته است.
در هنگام فلکشن و اکستنشن در مفصل تیبیوفمورال ترکیبی از حرکات رول، گلاید (اسلاید) و چرخش در سطح مفصل اتفاق میافتد که برای حفظ تجانس دو استخوان ران و درشتنی روی همدیگر در هنگام حرکت ضروری است [6]. در مفصل زانو در هنگام حرکت، نسبت مقادیر رول و گلاید از طریق بررسی مسیر مرکز لحظهای چرخش استنباط میشود [7-10]. درواقع عملکرد اصلی رباط متقاطع قدامی ایجاد ثبات در حرکات انتقالی و چرخش تیبیا نسبت به فمور است [7، 10]. رباط متقاطع قدامی دارای دو باند قدامی داخلی و خلفی خارجی است. باند قدامی داخلی هنگامی که زانو به فلکشن میرود، سفت و محکم میشود و باند خلفی خارجی نیز در زمان اکستنشن زانو در حالت سفت و محکم قرار میگیرد. این ترتیب عملکرد در رباط متقاطع قدامی نشاندهنده اعمال نقش این رباط در سرتاسر دامنه حرکتی فلکشن و اکستنشن است [8].
همچنین رباط متقاطع قدامی، نگهدارنده اصلی جابهجایی قدامی تیبیا روی فمور در حرکت هایپر اکستنش و همچنین جلوگیریکننده از واروس و والگوس زانو در هنگام اکستنش کامل است. همچنین این رباط از چرخش داخلی و خارجی زانو نیز در هنگام اکستنشِ کامل جلوگیری میکند [11]. البته باید اشاره شود که با ابداع تکنولوژیهای پیشرفته، میزان این حرکات به میلیمتر به شکل بسیار دقیق اندازهگیری شده است که نتایج آنها به ما نشان میدهد درک آرتروکینماتیک مفصل تیبیوفمورال از آنچه تصور میشود، پیچیدهتر است. برای نمونه خاصیان و همکاران به وسیله فلورسکوپی به روش دوبُعدی و سهبُعدی، گزارش کردند که از اکستنش کامل تا حداکثر فلکشن زانو در خلف اپیکندیل خارجی ران به طور متوسط 2±2/5 میلیمتر رول خلفی و در اپیکندیل داخلی به مقدار 2/2 ± 2/5 میلیمتر رول قدامی ایجاد میشود [12].
مطالعات گذشته ثابت کردهاند که حتی رباط متقاطع قدامی آسیبدیده که بازسازی شده است، نشانههایی از بیثباتی را نشان میدهد [13-21]. با توجه به نقش محوری رباط متقاطع قدامی در کنترل ثبات و پایداری مفصل زانو [22]، ثابت شده است پارگی آن منجر به کاهش حس عمقی، تعادل، قدرت، عملکرد عضلانی و همانطور که اشاره شد، تغییرات بیومکانیکی خواهد شد [23]. همچنین در اثر آسیب این رباط الگوی بارهای واردشده بر سطوح مفصلی تغییر خواهد کرد. تغییر این الگو باعث ورود بارهای غیرطبیعی روی غضروف سطوح مفصلی در طی فعالیتهای عملکردی شده و درنهایت این تغییرات منجر به تخریب سطوح غضروف و بروز یا پیشرفت استئوآرتریت میشود [24، 25]. فهم دقیق تغییرات جزئی آرتروکینماتیکی حاصل از پارگی رباط متقاطع قدامی اینجا هم اهمیت پیدا میکند که طبق گزارش بارینیوس و همکاران حتی بعد از بازسازی رباط متقاطع قدامی نیز 57 درصد از افرادی که طی چهارده سال تحت نظر بودند، در زانوی آسیبدیده دچار پیشرفت استئوآرتریت شده بودند [26]. موارد اشارهشده این پرسش را ایجاد میکند که مگر بعد از پارگی رباط متقاطع قدامی و حتی بعد از بازسازی آن چه تغییرات آرتروکینماتیکی رخ میدهد که این تغییرات باعث عوارض برگشتناپذیر میشود؟ متأسفانه هیچ مقاله مروری داخلی و خارجیای نیافتیم که این سؤال را در قالب جامعتر و دقیقتری پاسخ دهد؛ بنابراین هدف از تحقیق مروری حاضر پی بردن به مهمترین تغییرات آرتروکینماتیکی بعد از پارگی رباط متقاطع قدامی (چه قبل و چه بعد از بازسازی و همچنین بعد از یک دوره توانبخشی) با توجه به تحقیقات گذشته است.
روششناسی
در این مقاله مروری سعی کردیم مطالعات انجامشده در زمینه تغییرات آرتروکینماتیک زانوی دارای آسیب رباط متقاطع قدامی قبل و بعد از بازسازی نسبت به زانوی سالم را از سال 1970 تا 2020 جمعآوری کنیم. این مقالات را با جستوجو در وبسایتهای وب آو ساینس، گوگل اسکالر، ساینس دایرکت، اسکوپوس، پابمد، مد لاین، پدرو، سینال، اسپورت دیسکاس، امبیس گردآوری کردیم. واژگان کلیدی استفادهشده در این جستوجو شامل موارد زیر و مترادف آنها میشود:
Biomechanics of the knee joint, Gait knee kinematics, Knee َarthrokinematics, Anterior cruciate ligament deficient, Injured anterior cruciate ligaments, Sagittal plane knee motion, ACL reconstruction, Knee pathology, Knee joint movements, Accessory movement, Knee hypermobility.
همچنین برای جستوجوی مقالات فارسی در پایگاه اطلاعات علمی جهاد دانشگاهی، پایگاه استنادی علوم جهان اسلام، پایگاه مجلات کشور، پایگاه پژوهشگاه علوم و فناوری اطلاعات ایران، بانک مقالات سلامت، بانک جامع مقالات پزشکی از کلیدواژههای کینماتیک مفصل زانو، آرتروکینماتیک مفصل زانو، آرتروکینماتیک زانو بعد از پارگی و بازسازی رباط متقاطع قدامی، حرکات فرعی مفصل زانو و حرکات انتقالی مفصل زانو استفاده کردیم. از کلیدواژههای انگلیسی یادشده برای پیداکردن مقالات انگلیسی چاپشده در مجلات علمی داخلی استفاده شد. از جستوجوی دستی نیز برای یافتن مقالات استفاده کردیم.
در این بررسی کیفیت مقالات با جدول چکلیست تعدیلشده داون و بلک امتیازدهی شد [27] (جدول شماره 1).

درواقع این چکلیست برای ارزیابی روششناسی مقالات تصادفی و غیرتصادفی تنظیم شده است. در این چکلیست 27 سؤال وجود دارد. بخش اول گزارشدهی شامل ده سؤال، بخش دوم اعتبار بیرونی شامل سه سؤال، بخش سوم اعتبار داخلی (که خود به دو قسمت سوگیری و مداخلهگر تقسیم میشود) شامل چهارده سؤال است؛ برای مثال در قسمت گزارشدهی پرسیده شده است که آیا فرضیهها، اهداف تحقیق و یا مداخلات مدنظر بهروشنی توضیح داده شده است؟ بر اساس این چکلیست مقالات در چهار سطح قرار میگیرند. اگر نمره مقالهای بین 24 تا 28 بود در سطح عالی، 19 تا 23 سطح خوب، 14 تا 18 سطح نسبتاً خوب و اگر کمتر از 13 بود در سطح ضعیف قرار میگرفت [28].
عنوان و چکیده هر مطالعه جداگانه توسط نویسنده ارزیابی شد. اولین مرحله در انتخاب مقالات بر اساس این موضوع بود که آیا چکیده یا عنوان مقاله با موضوع تحقیق همخوانی دارد یا خیر. مراحل بعدی انتخاب مقالات مطابق با معیارهای زیر بود:
1. مطالعاتی که به زبان انگلیسی و فارسی منتشر شدهاند؛
2. متن کامل مقاله در دسترس باشد؛
3. مطالعاتی که حرکات آرتروکینماتیک مفصل زانو را بعد از پارگی رباط متقاطع قدامی بررسی کرده باشند؛
4. مطالعاتی که حرکات آرتروکینماتیک زانو را بعد از ترمیم رباط متقاطع قدامی پارهشده ارزیابی کرده باشند؛
5. مطالعاتی که حرکات آرتروکینماتیک زانو را بعد از یک دوره توانبخشی بررسی کرده باشند.
و همچنین تحقیقاتی که نقش آرتروکینماتیکی دیگر ساختارهای زانو و یا مفاصل دیگر را مورد بررسی قرار داده بودند از مسیر بررسی حذف گردیدند.

Biomechanics of the knee joint, Gait knee kinematics, Knee َarthrokinematics, Anterior cruciate ligament deficient, Injured anterior cruciate ligaments, Sagittal plane knee motion, ACL reconstruction, Knee pathology, Knee joint movements, Accessory movement, Knee hypermobility.
همچنین برای جستوجوی مقالات فارسی در پایگاه اطلاعات علمی جهاد دانشگاهی، پایگاه استنادی علوم جهان اسلام، پایگاه مجلات کشور، پایگاه پژوهشگاه علوم و فناوری اطلاعات ایران، بانک مقالات سلامت، بانک جامع مقالات پزشکی از کلیدواژههای کینماتیک مفصل زانو، آرتروکینماتیک مفصل زانو، آرتروکینماتیک زانو بعد از پارگی و بازسازی رباط متقاطع قدامی، حرکات فرعی مفصل زانو و حرکات انتقالی مفصل زانو استفاده کردیم. از کلیدواژههای انگلیسی یادشده برای پیداکردن مقالات انگلیسی چاپشده در مجلات علمی داخلی استفاده شد. از جستوجوی دستی نیز برای یافتن مقالات استفاده کردیم.
در این بررسی کیفیت مقالات با جدول چکلیست تعدیلشده داون و بلک امتیازدهی شد [27] (جدول شماره 1).

درواقع این چکلیست برای ارزیابی روششناسی مقالات تصادفی و غیرتصادفی تنظیم شده است. در این چکلیست 27 سؤال وجود دارد. بخش اول گزارشدهی شامل ده سؤال، بخش دوم اعتبار بیرونی شامل سه سؤال، بخش سوم اعتبار داخلی (که خود به دو قسمت سوگیری و مداخلهگر تقسیم میشود) شامل چهارده سؤال است؛ برای مثال در قسمت گزارشدهی پرسیده شده است که آیا فرضیهها، اهداف تحقیق و یا مداخلات مدنظر بهروشنی توضیح داده شده است؟ بر اساس این چکلیست مقالات در چهار سطح قرار میگیرند. اگر نمره مقالهای بین 24 تا 28 بود در سطح عالی، 19 تا 23 سطح خوب، 14 تا 18 سطح نسبتاً خوب و اگر کمتر از 13 بود در سطح ضعیف قرار میگرفت [28].
عنوان و چکیده هر مطالعه جداگانه توسط نویسنده ارزیابی شد. اولین مرحله در انتخاب مقالات بر اساس این موضوع بود که آیا چکیده یا عنوان مقاله با موضوع تحقیق همخوانی دارد یا خیر. مراحل بعدی انتخاب مقالات مطابق با معیارهای زیر بود:
1. مطالعاتی که به زبان انگلیسی و فارسی منتشر شدهاند؛
2. متن کامل مقاله در دسترس باشد؛
3. مطالعاتی که حرکات آرتروکینماتیک مفصل زانو را بعد از پارگی رباط متقاطع قدامی بررسی کرده باشند؛
4. مطالعاتی که حرکات آرتروکینماتیک زانو را بعد از ترمیم رباط متقاطع قدامی پارهشده ارزیابی کرده باشند؛
5. مطالعاتی که حرکات آرتروکینماتیک زانو را بعد از یک دوره توانبخشی بررسی کرده باشند.
و همچنین تحقیقاتی که نقش آرتروکینماتیکی دیگر ساختارهای زانو و یا مفاصل دیگر را مورد بررسی قرار داده بودند از مسیر بررسی حذف گردیدند.

نتایج
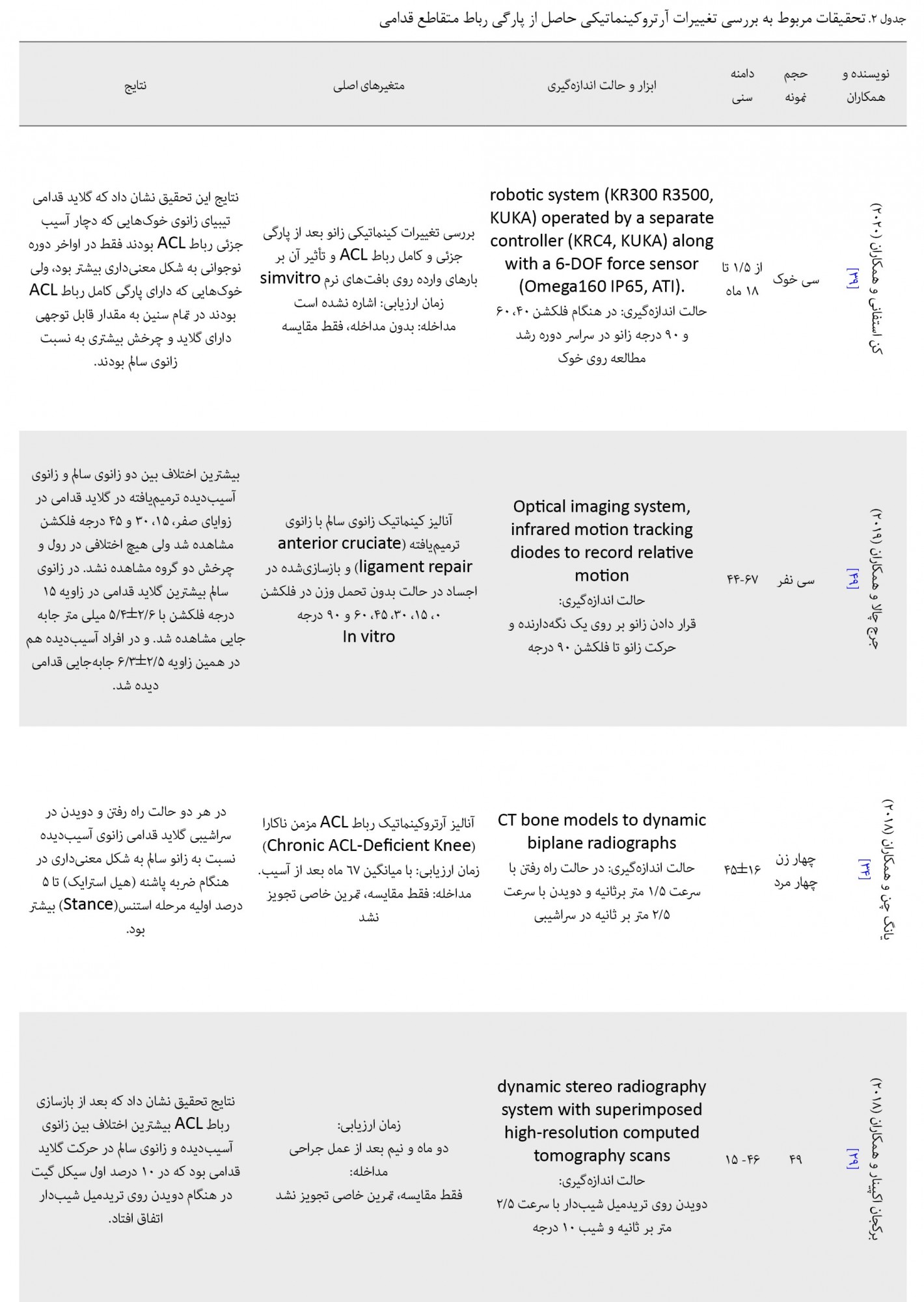
پس از غربالگری بر اساس عنوان، چکیده مقاله و موارد تکراری، مقالاتیکه با هدف مطالعه تناسب نداشتند، حذف شدند. درنهایت بر اساس معیارهای تحقیق بیست مقاله برای بررسی انتخاب شد. از تحقیقات یافتشده هشت تحقیق، آرتروکینماتیک زانو را در هنگام راه رفتن و دویدن در حالت عادی یا در سراشیبی روی تریدمیل ارزیابی کرده بودند [29-36]. هفت تحقیق، آرتروکینماتیک زانو را در حالت ایستا و تحمل وزن روی یک پا انجام داده بودند [37-43]. دو تحقیق در حالت بالا و پایین رفتن از پله [44-46]، یک تحقیق روی ترامپولین در حالت شیفت دادن بدن به یک طرف [47]، یک تحقیق دیگر نیز در حالت آزمون لاچمن [48] بررسی کرده بودند. یک تحقیق باقیمانده نیز ارزیابی آرتروکینماتیکی مفصل زانو را بعد از پارگی روی اجساد انجام داده بود [49].
پنج تحقیق، متغیرهای کینماتیکی خود را قبل و بعد از بازسازی رباط متقاطع قدامی ارزیابی و مقایسه کرده بودند [29، 32، 35، 36، 43، 45، 46، 48، 49]. همانطور که در جدول شماره 2 مشاهده میشود، از بیست مقاله بررسیشده شش مقاله از سیستم آنالیز سهبعدی حرکت [30، 33، 35، 36، 41، 46]، چهار مقاله از دستگاه فلورسکوپی [38، 40، 42، 48]، دو مقاله از روش سیتی اسکن استخوان [32، 34]، دو مقاله دیگر نیز از روش داینامیک رادیو استریومتری [37، 45] و مقالات دیگر نیز هرکدام به روشهای متفاوت دیگر ازجمله استریوفتوگرامتریک، داینامیک استریو رادیوگرافیک سیستم، داینامیک رادیوگرافیک ایکسری و چند روش دیگر برای ارزیابی متغیرهای آرتروکینماتیکی مفصل زانو استفاده کردهاند. تکنیک آنالیز سهبعدی حرکت درواقع تکنیکی است که با استفاده از تجهیزاتی مانند دوربین و لندمارکها و همچنین نرمافزارهای مخصوص حرکات مفاصل را در فضای سهبُعدی تهیه میکند [35]. همچنین روش فلورسکوپی که در کنار روش آنالیز سهبعدیِ حرکت، پرکاربردترین ابزار برای اندازهگیری آرتروکینماتیک مفصل زانو در مقالات بود، یک تکنیک تصویربرداری است که با تاباندن پرتو اشعه ایکس تصویر متحرکی را از ساختارهای درونی بیمار تهیه میکند [40].

.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
اینکه ارزیابیها چه مدت بعد از پارگی یا چه مدت بعد از ترمیم یا بازسازی صورت گرفته باشد، کمی متفاوت است. شش مقاله ارزیابیهای خود را یک تا سه ماه بعد از پارگی یا بازسازی [29، 35، 36، 45، 46، 48]، شش مقاله سه تا شش ماه [32، 33، 38، 40-42]، سه مقاله نیز شش تا نه ماه بعد از پارگی یا بازسازی [31، 37، 43] و سه مقاله دیگر نیز ارزیابیهای خود را بعد از نه ماه یا بیشتر انجام داده بودند [30، 34، 47]. همچنین با توجه به جدول شماره 1 بررسی سطحبندی مقالات بر اساس چکلیست تعدیلشده داون و بلک نشان داد که از بیست مقاله، نوزده مقاله در دامنه 19 تا 23 قرار گرفتهاند که نشاندهنده سطح خوب این مقالات بود و یک مقاله نیز با تعلق نمره 24 به خود و قرار گرفتن در دامنه 24 تا 28 در سطح عالی رتبهبندی شد.
در انتها نیز باید اشاره شود که دو مقاله هوشینو و همکاران [32] و گا او بو و همکاران [46] نیز به تأثیر یک دوره برنامه ششماهه توانبخشی روی حرکات آرتروکینماتیک رباط متقاطع قدامی بعد از بازسازی پرداخته بودند. در جدول شماره 2 خلاصه یافتههای تحقیقات ذکر شده است.
پنج تحقیق، متغیرهای کینماتیکی خود را قبل و بعد از بازسازی رباط متقاطع قدامی ارزیابی و مقایسه کرده بودند [29، 32، 35، 36، 43، 45، 46، 48، 49]. همانطور که در جدول شماره 2 مشاهده میشود، از بیست مقاله بررسیشده شش مقاله از سیستم آنالیز سهبعدی حرکت [30، 33، 35، 36، 41، 46]، چهار مقاله از دستگاه فلورسکوپی [38، 40، 42، 48]، دو مقاله از روش سیتی اسکن استخوان [32، 34]، دو مقاله دیگر نیز از روش داینامیک رادیو استریومتری [37، 45] و مقالات دیگر نیز هرکدام به روشهای متفاوت دیگر ازجمله استریوفتوگرامتریک، داینامیک استریو رادیوگرافیک سیستم، داینامیک رادیوگرافیک ایکسری و چند روش دیگر برای ارزیابی متغیرهای آرتروکینماتیکی مفصل زانو استفاده کردهاند. تکنیک آنالیز سهبعدی حرکت درواقع تکنیکی است که با استفاده از تجهیزاتی مانند دوربین و لندمارکها و همچنین نرمافزارهای مخصوص حرکات مفاصل را در فضای سهبُعدی تهیه میکند [35]. همچنین روش فلورسکوپی که در کنار روش آنالیز سهبعدیِ حرکت، پرکاربردترین ابزار برای اندازهگیری آرتروکینماتیک مفصل زانو در مقالات بود، یک تکنیک تصویربرداری است که با تاباندن پرتو اشعه ایکس تصویر متحرکی را از ساختارهای درونی بیمار تهیه میکند [40].
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
اینکه ارزیابیها چه مدت بعد از پارگی یا چه مدت بعد از ترمیم یا بازسازی صورت گرفته باشد، کمی متفاوت است. شش مقاله ارزیابیهای خود را یک تا سه ماه بعد از پارگی یا بازسازی [29، 35، 36، 45، 46، 48]، شش مقاله سه تا شش ماه [32، 33، 38، 40-42]، سه مقاله نیز شش تا نه ماه بعد از پارگی یا بازسازی [31، 37، 43] و سه مقاله دیگر نیز ارزیابیهای خود را بعد از نه ماه یا بیشتر انجام داده بودند [30، 34، 47]. همچنین با توجه به جدول شماره 1 بررسی سطحبندی مقالات بر اساس چکلیست تعدیلشده داون و بلک نشان داد که از بیست مقاله، نوزده مقاله در دامنه 19 تا 23 قرار گرفتهاند که نشاندهنده سطح خوب این مقالات بود و یک مقاله نیز با تعلق نمره 24 به خود و قرار گرفتن در دامنه 24 تا 28 در سطح عالی رتبهبندی شد.
در انتها نیز باید اشاره شود که دو مقاله هوشینو و همکاران [32] و گا او بو و همکاران [46] نیز به تأثیر یک دوره برنامه ششماهه توانبخشی روی حرکات آرتروکینماتیک رباط متقاطع قدامی بعد از بازسازی پرداخته بودند. در جدول شماره 2 خلاصه یافتههای تحقیقات ذکر شده است.
بحث
بعد از پارگی رباط متقاطع قدامی مهمترین و بارزترین تغییر آرتروکینماتیکی که ممکن است در خیلی از افراد در بعضی از آزمونها مانند تست لاچمن دیده شود، افزایش حرکت قدامی استخوان درشتنی نسبت به استخوان ران است [48]. با توجه به جدول شماره 2 بررسیهای تحقیق حاضر نیز نشان میدهد که پانزده تحقیق از بیست تحقیق یافتشده گزارش کردهاند که گلاید قدامی در زانوی آسیبدیده نسبت به زانوی سالم به شکل معنیداری افزایش یافته است. در پنج تحقیق باقیمانده سه تحقیق در گلاید قدامی بین دو گروه آسیبدیده و سالم اختلاف معنیداری مشاهده نکردند [33، 36، 37] و یک تحقیق دیگر نیز گلاید زانو را بررسی نکرده بود [46]. تنها تحقیقی که برخلاف تحقیقات دیگر به شکل معنیدار در افراد آسیبدیده به نسبت افراد سالم گلاید قدامی کمتری مشاهده کرده بود، تحقیق توماس آندریاچی و همکاران بود [30]. شاید بتوان تفاوت نتیجه مقاله آندریاچی و همکاران با سایر مقالات را در این دید که آنها بررسی روی افراد آسیبدیده را بر خلاف سایر مقالات خیلی دیرتر، یعنی با میانگین 127 ماه بعد از آسیب، آغاز کردند. چون هدف آنها بررسی تغییرات الگوی فراخوانی عضلات، در نتیجه تغییرات کینماتیکی زانوی دارای رباط متقاطع قدامی آسیبدیده، بعد از گذشت حدود 127 ماه بود.
در بین مقالات این اتفاق نظر دیده میشود که بیشترین اختلاف آرتروکینماتیکی مشاهدهشده در افراد آسیبدیده به نسبت افراد سالم، بین پانزده درجه فلکشن و اکستنشن کامل زانو اتفاق میافتد [29، 38، 40، 42، 49، 50].
نکته مهم دیگری که باید به آن توجه کرد این است که حرکات آرتروکینماتیکی رخداده در مفصل زانو بین اپیکندیل داخلی و اپیکندیل خارجی متفاوت است. هوشینو و همکاران، داگلاس و همکاران و همچنین سانگبوم و همکاران اشاره کردهاند که تغییرات در گلاید قدامی در افراد دارای آسیب رباط متقاطع قدامی به نسبت افراد سالم در اپیکندیل داخلی بیشتر از اپیکندیل خارجی اتفاق افتاده است [32، 41، 48]، ولی کینین و همکارانش اشاره کردهاند که اختلاف گلاید قدامی زانوی آسیبدیده به نسبت زانوی سالم در اپیکندیل خارجی، بیشتر از اپیکندیل داخلی اتفاق افتاده است [38]. کینین و همکارانش بر خلاف سه تحقیق دیگر این تغییرات را در حالت نزدیک به اکستنش مشاهده کردند؛ در حالی که داگلاس و سانگبوم ازریابیهای خود را در حالت فلکشن، و هوشینو در حالت دویدن روی تریدمیل انجام دادند.
متغیر آرتروکینماتیکی دیگری که در مقالات بین دو گروه چشمگیر به نظر میرسد تغییرات مربوط به چرخش بود. براندسون و همکاران، یو ژانگ و همکاران، کینین و همکاران، جانسون و همکاران و همچنین سانگبوم و همکاران اشاره کردهاند که در زانوی آسیبدیده به نسبت زانوی سالم در حرکات مشخص، چرخش خارجی بیشتری رخ داده یا چرخش داخلی به شکل معنیداری کاهش یافته است [37، 38، 43، 46، 48]. ولی آندریاچی و همکاران (2005) به این نتیجه رسیدند که در افراد آسیبدیده چرخش خارجی کاهش یافته [30] و نتایج تحقیق دفریت و همکاران و ژانگ و همکاران (2010) نیز نشان داد که در افراد آسیبدیده چرخش داخلی افزایش یافته است [40، 46]. شاید میتوان اختلاف نتایج را در اینجا دید که دفریت و همکاران و آندریاچی و همکاران این اختلاف بین دو گروه را در نزدیکی اکستنش مشاهده کردند، ولی براندسون و همکاران، جانسون و همکاران، ژانگ و همکاران و همچنین سانگبوم و همکاران این اختلاف را در زوایای 30 درجه به بالا در فلکشن زانو مشاهده کردند.
آزمون ارزیابی یو ژانگ و همکاران نیز کاملاً با بقیه متفاوت بود. آنها ارزیابی آرتروکینماتیک زانوی آسیبدیده را در حال بالا و پایین رفتن از پله بررسی کردند.
البته به این نکته بسیار مهم نیز باید اشاره کرد که از بین پانزده تحقیق مذکور، پنج تحقیقی که زانوی آسیبدیده را بعد از بازسازی مطالعه کردند، به این نکته اشاره کردند که در تغییرات آرتروکینماتیکی رخداده در قبل و بعد از بازسازی رباط متقاطع قدامی اختلاف معنیداری مشاهده نشده است و زانوی دارای رباط بازسازیشده به نسبت زانوی سالم به شکل معنیداری دارای گلاید قدامی بیشتری است. البته باید به این نکته نیز اشاره شود که براندسون و همکاران گزارش کردهاند با بازسازی رباط، گلاید قدامی و بعضی از متغیرهای آرتروکینماتیکی بهخصوص گلاید داخلی، ممکن است به مقدار خیلی اندکی نسبت به قبل از عمل بازسازی کاهش یابد، ولی با وجود این، هنوز نسبت به پای سالم این اختلاف معنیدار است.
اینکه تحقیقات بررسیشده تغییرات آرتروکینماتیکی زانو را با چه فاصله زمانی بعد از آسیب یا بعد از بازسازی بررسی کنند، مهم است. همانطور که در قسمت نتایج اشاره شد، از بیست تحقیق بررسیشده فقط سه تحقیق چن یانگ و همکاران [34]، کویست و همکاران [47] و آندریاچی و همکاران [30] تغییرات آرتروکینماتیک زانو را به ترتیب 67، 26 و 127 ماه بعد از آسیب بررسی کردند. چون یکی از اهداف این سه تحقیق، بررسی تأثیر درازمدت یک رباط متقاطع آسیبدیده و ناکارآمد، بدون اینکه بازسازی شود، روی آرتروکینماتیک مفصل زانو بوده است. البته هدف اصلی این سه تحقیق که خواستهاند بعد از گذشت این مدت طولانی تغییرات آرترو کینماتیکی را بررسی کنند، این بوده است که تأثیر این تغییرات را در درازمدت روی عضلات و الگوی فراخوانی آنها بررسی کنند. هر سه تحقیق به این نتیجه رسیدهاند که به دلیل تغییر حرکات آرتروکینماتیکی مفصل زانو در این افراد بهخصوص تغییر در گلاید قدامی و همچنین تغییر در چرخش مفصل تیبیوفمورال در هنگام راه رفتن، دویدن و شیفت دادن بدن به جلو و عقب، علاوه بر تغییر در الگوی فراخوانی عضلات، مسیر تماس تیبیا و فمور روی همدیگر تغییر یافته و این امر میتواند منجر به انواع تغییرات تخریبی (دژنراتیو) گزارششده در منیسک و غضروف مفصلی باشد [30، 34، 47]. البته باید اشاره کرد که در تحقیق یانگ چن و همکاران میانگین سن افراد بررسیشده 45 سال، در تحقیق کویست و همکاران 28 سال و در تحقیق آندریاچی و همکاران 37 سال بود.
به علاوه باید اشاره شود که پانزده تحقیق دیگر که هدف اصلی آنها نه بررسی تغییرات تخریبی مفصل، بلکه تنها بررسی تغییرات آرتروکینماتیکی حاصل از پارگی رباط متقاطع قدامی بوده است، این ارزیابیها را حداکثر نه ماه بعد از آسیب یا بازسازی رباط انجام دادهاند (دو تحقیق باقیمانده روی جسد و روی خوک انجام شده بود).
آخرین و شاید یکی از مهمترین نکاتی که در مورد افراد دارای پارگی رباط متقاطع قدامی از اهمیت زیادی برخوردار است و متأسفانه کمتر بدان توجه شده است، پیدا کردن گلاید داخلی تیبیا در این افراد است. دفریت و همکاران [40] اشاره کردند که بعد از پارگی رباط متقاطع قدامی، استخوان تیببا در فلکشن 15 تا 90 درجه، حدود 1 میلیمتر، به سمت داخل گلاید پیدا میکند و این جابهجایی باعث تغییر توزیع فشار در غضروف تیبیوفمورال در نزدیکی خار داخلی تیبیا میشود. در ادامه آنها اشاره میکنند که این یافتهها با مشاهدات فیرکلاف و همکاران [51] ارتباط دارد؛ آنها در مشاهدات خود استئوآرتریت را در این ناحیه میان افرادی که دچار پارگی مزمن رباط متقاطع قدامی شده بودند، مشاهده کردند. در انتها دفریت و همکاران پیشنهاد کردهاند که در برنامه توانبخشی افراد دچار پارگی ACL، همچنین در تکنیکهای بازسازی این رباط علاوه بر ثبات قدامی خلفی به ثبات داخلی خارجی نیز توجه کافی شود. همچنین باید اشاره شود که هوشینو و همکاران، هیون و همکاران، یو ژانگ و همکاران و براتدسون همکاران [32، 35، 36، 45] نیز در افرادی که دچار پارگی رباط ACL شده بودند نیز این گلاید داخلی را مشاهده کردند.
در انتها به این نکته باید اشاره کنیم که از بیست تحقیق بررسیشده دو تحقیق تأثیر تمرینات توانبخشی را روی تغییرات آرتروکینماتیکی زانوی دارای رباط متقاطع بازسازیشده، بررسی کردند. هوشینو و همکاران تأثیر یک دوره تمرینات دامنه حرکتی و تمرینات قدرتی که به مدت حداکثر نه ماه ادامه پیدا کرد را روی آرتروکینماتیک زانوی بازسازیشده، هنگام دویدن در سراشیبی ارزیابی کردند؛ نتیجه تحقیقات آنها حاکی از این بود که حتی بعد از دوره توانبخشی نیز این افراد در مرحله ضربه پاشنه (هیل استرایک) در هنگام دویدن در سراشیبی به نسبت افراد سالم در مفصل زانو حرکات رول و گلاید بیشتری داشتند [32].
گا اوبو و همکاران نیز برای افرادی که رباط متقاطع قدامی خود را بازسازی کرده بودند یک دوره تمرینات توانبخشی ششمرحلهای شامل تمرینات حمایتی (یک تا هفت روز بعد از عمل)، تمرینات مربوط به تحرک اولیه (هشت تا بیست روز)، حرکات کنترلشده (سه تا شش هفته)، حرکات قدرتی و حس عمقی پیشرفته (هفت تا ده هفته)، تمرینات پلایومتریک و دویدن (یازده تا دوازده هفته) و تمرینات چابکی (سیزده هفته تا شش ماه) را به مدت شش ماه تجویز کردند. نتایج این تحقیق نشان داد متغیرهای کینماتیکی زانوی بازسازی شده علیرغم شرکت در یک برنامه توانبخشی شباهت بیشتری به زانوی آسیبدیده بازسازینشده دارد تا زانوی سالم [46]. در همین راستا هرمان فورماین و همکارانش نیز در تحقیق خود به این نتیجه رسیدهاند، در افرادی که رباط متقاطع خود را بازسازی کردهاند علیرغم شرکت در پروتکل توانبخشی بروز آسیب مجدد در رباط متقاطع قدامی به طور توجهبرانگیزی افزایش یافته است [52]. اینکه چرا بازسازی رباط و متعاقب آن برنامههای توانبخشی نتوانستهاند نتایج مورد انتظار را ایجاد کنند سؤال مهمی است که در مقاله مروری کریستوفر ناجلی و همکارش به آن پرداخته شده است. مقاله مروری آنها با این سؤال شروع میشود که بر اساس ملاحظات زیستشناختی و عملکردی آیا بعد از بازسازی رباط متقاطع قدامی بازگشت به فعالیت ورزشی را باید دو سال به تأخیر انداخت؟ آنها بیان داشتهاند بعد از پارگی رباط و بازسازی آن، چند نکته را باید مورد توجه قرار داد: 1. بعد از بروز آسیب و بازسازی رباط تکثیر سلولهای عروق خونی و عصبی با سرعت کمتری نسبت به مدت زمانی که ورزشکاران به فعالیت بازمیگردند که معمولاًًً بین شش تا دوازده ماه است رخ میدهد [53-56]؛ 2. اغلب اوقات متعاقب آسیب رباط متقاطع قدامی، غضروف و استخوان زیرغضروف نیز به طور توجهبرانگیزی آسیب میبیند [57-60]؛ 3. گیرندههای حسی و میکانیکی سه درصد از حجم بافت رباط را تشکیل میدهند و بین آنها و عضلات اطراف مفصل یک حلقه رفلکسی ایجادشده که به ثبات داینامیک مفصل و حس عمقی آن کمک میکند. زمانی که رباط متقاطع قدامی دچار پارگی میشود، عملکرد حسی کاهش مییابد که علیرغم بازسازی رباط این اختلال عملکرد باقی میماند [61-64]؛ 4. هرچند توانبخشی میتواند بعد از عمل، باعث کاهش افیوژن مفصلی، بهبود دامنه حرکتی و همچنین بهبود قدرت و عملکرد عضله چهارسر شود، ولی به طور خاص ورزشکارانی که رباط خود را بازسازی کردهاند، در کنترل عصبیعضلانی و قدرت اکستنش زانو دارای ویژگیهای مشخصی هستند که تا دو سال بعد از بازسازی به سطح پایه نمیرسند [65-70].
ناجلی و همکارش در انتها به این نتیجه رسیدهاندکه شواهد موجود در ادبیات پیشینه نشان میدهد برای رسیدن به سلامت پایه مفصل بعد از بازسازی رباط و انجام یک دوره توانبخشی در ورزشکاران به حدود دو سال وقت نیاز است و پیشنهاد دادهاند بهتر است، ورزشکارانی که رباط متقاطع قدامی خود را بازسازی کردهاند بهخصوص ورزشکاران جوانتر تا دو سال به فعالیت اصلی خود بازنگردند؛ زیرا بررسی آنها نشان داد تأخیر در بازگشت به فعالیت اصلی تقریباً برای دو سال به طور توجهبرانگیزی بروز آسیب بعدی در این رباط را کاهش میدهد [71].
در بین مقالات این اتفاق نظر دیده میشود که بیشترین اختلاف آرتروکینماتیکی مشاهدهشده در افراد آسیبدیده به نسبت افراد سالم، بین پانزده درجه فلکشن و اکستنشن کامل زانو اتفاق میافتد [29، 38، 40، 42، 49، 50].
نکته مهم دیگری که باید به آن توجه کرد این است که حرکات آرتروکینماتیکی رخداده در مفصل زانو بین اپیکندیل داخلی و اپیکندیل خارجی متفاوت است. هوشینو و همکاران، داگلاس و همکاران و همچنین سانگبوم و همکاران اشاره کردهاند که تغییرات در گلاید قدامی در افراد دارای آسیب رباط متقاطع قدامی به نسبت افراد سالم در اپیکندیل داخلی بیشتر از اپیکندیل خارجی اتفاق افتاده است [32، 41، 48]، ولی کینین و همکارانش اشاره کردهاند که اختلاف گلاید قدامی زانوی آسیبدیده به نسبت زانوی سالم در اپیکندیل خارجی، بیشتر از اپیکندیل داخلی اتفاق افتاده است [38]. کینین و همکارانش بر خلاف سه تحقیق دیگر این تغییرات را در حالت نزدیک به اکستنش مشاهده کردند؛ در حالی که داگلاس و سانگبوم ازریابیهای خود را در حالت فلکشن، و هوشینو در حالت دویدن روی تریدمیل انجام دادند.
متغیر آرتروکینماتیکی دیگری که در مقالات بین دو گروه چشمگیر به نظر میرسد تغییرات مربوط به چرخش بود. براندسون و همکاران، یو ژانگ و همکاران، کینین و همکاران، جانسون و همکاران و همچنین سانگبوم و همکاران اشاره کردهاند که در زانوی آسیبدیده به نسبت زانوی سالم در حرکات مشخص، چرخش خارجی بیشتری رخ داده یا چرخش داخلی به شکل معنیداری کاهش یافته است [37، 38، 43، 46، 48]. ولی آندریاچی و همکاران (2005) به این نتیجه رسیدند که در افراد آسیبدیده چرخش خارجی کاهش یافته [30] و نتایج تحقیق دفریت و همکاران و ژانگ و همکاران (2010) نیز نشان داد که در افراد آسیبدیده چرخش داخلی افزایش یافته است [40، 46]. شاید میتوان اختلاف نتایج را در اینجا دید که دفریت و همکاران و آندریاچی و همکاران این اختلاف بین دو گروه را در نزدیکی اکستنش مشاهده کردند، ولی براندسون و همکاران، جانسون و همکاران، ژانگ و همکاران و همچنین سانگبوم و همکاران این اختلاف را در زوایای 30 درجه به بالا در فلکشن زانو مشاهده کردند.
آزمون ارزیابی یو ژانگ و همکاران نیز کاملاً با بقیه متفاوت بود. آنها ارزیابی آرتروکینماتیک زانوی آسیبدیده را در حال بالا و پایین رفتن از پله بررسی کردند.
البته به این نکته بسیار مهم نیز باید اشاره کرد که از بین پانزده تحقیق مذکور، پنج تحقیقی که زانوی آسیبدیده را بعد از بازسازی مطالعه کردند، به این نکته اشاره کردند که در تغییرات آرتروکینماتیکی رخداده در قبل و بعد از بازسازی رباط متقاطع قدامی اختلاف معنیداری مشاهده نشده است و زانوی دارای رباط بازسازیشده به نسبت زانوی سالم به شکل معنیداری دارای گلاید قدامی بیشتری است. البته باید به این نکته نیز اشاره شود که براندسون و همکاران گزارش کردهاند با بازسازی رباط، گلاید قدامی و بعضی از متغیرهای آرتروکینماتیکی بهخصوص گلاید داخلی، ممکن است به مقدار خیلی اندکی نسبت به قبل از عمل بازسازی کاهش یابد، ولی با وجود این، هنوز نسبت به پای سالم این اختلاف معنیدار است.
اینکه تحقیقات بررسیشده تغییرات آرتروکینماتیکی زانو را با چه فاصله زمانی بعد از آسیب یا بعد از بازسازی بررسی کنند، مهم است. همانطور که در قسمت نتایج اشاره شد، از بیست تحقیق بررسیشده فقط سه تحقیق چن یانگ و همکاران [34]، کویست و همکاران [47] و آندریاچی و همکاران [30] تغییرات آرتروکینماتیک زانو را به ترتیب 67، 26 و 127 ماه بعد از آسیب بررسی کردند. چون یکی از اهداف این سه تحقیق، بررسی تأثیر درازمدت یک رباط متقاطع آسیبدیده و ناکارآمد، بدون اینکه بازسازی شود، روی آرتروکینماتیک مفصل زانو بوده است. البته هدف اصلی این سه تحقیق که خواستهاند بعد از گذشت این مدت طولانی تغییرات آرترو کینماتیکی را بررسی کنند، این بوده است که تأثیر این تغییرات را در درازمدت روی عضلات و الگوی فراخوانی آنها بررسی کنند. هر سه تحقیق به این نتیجه رسیدهاند که به دلیل تغییر حرکات آرتروکینماتیکی مفصل زانو در این افراد بهخصوص تغییر در گلاید قدامی و همچنین تغییر در چرخش مفصل تیبیوفمورال در هنگام راه رفتن، دویدن و شیفت دادن بدن به جلو و عقب، علاوه بر تغییر در الگوی فراخوانی عضلات، مسیر تماس تیبیا و فمور روی همدیگر تغییر یافته و این امر میتواند منجر به انواع تغییرات تخریبی (دژنراتیو) گزارششده در منیسک و غضروف مفصلی باشد [30، 34، 47]. البته باید اشاره کرد که در تحقیق یانگ چن و همکاران میانگین سن افراد بررسیشده 45 سال، در تحقیق کویست و همکاران 28 سال و در تحقیق آندریاچی و همکاران 37 سال بود.
به علاوه باید اشاره شود که پانزده تحقیق دیگر که هدف اصلی آنها نه بررسی تغییرات تخریبی مفصل، بلکه تنها بررسی تغییرات آرتروکینماتیکی حاصل از پارگی رباط متقاطع قدامی بوده است، این ارزیابیها را حداکثر نه ماه بعد از آسیب یا بازسازی رباط انجام دادهاند (دو تحقیق باقیمانده روی جسد و روی خوک انجام شده بود).
آخرین و شاید یکی از مهمترین نکاتی که در مورد افراد دارای پارگی رباط متقاطع قدامی از اهمیت زیادی برخوردار است و متأسفانه کمتر بدان توجه شده است، پیدا کردن گلاید داخلی تیبیا در این افراد است. دفریت و همکاران [40] اشاره کردند که بعد از پارگی رباط متقاطع قدامی، استخوان تیببا در فلکشن 15 تا 90 درجه، حدود 1 میلیمتر، به سمت داخل گلاید پیدا میکند و این جابهجایی باعث تغییر توزیع فشار در غضروف تیبیوفمورال در نزدیکی خار داخلی تیبیا میشود. در ادامه آنها اشاره میکنند که این یافتهها با مشاهدات فیرکلاف و همکاران [51] ارتباط دارد؛ آنها در مشاهدات خود استئوآرتریت را در این ناحیه میان افرادی که دچار پارگی مزمن رباط متقاطع قدامی شده بودند، مشاهده کردند. در انتها دفریت و همکاران پیشنهاد کردهاند که در برنامه توانبخشی افراد دچار پارگی ACL، همچنین در تکنیکهای بازسازی این رباط علاوه بر ثبات قدامی خلفی به ثبات داخلی خارجی نیز توجه کافی شود. همچنین باید اشاره شود که هوشینو و همکاران، هیون و همکاران، یو ژانگ و همکاران و براتدسون همکاران [32، 35، 36، 45] نیز در افرادی که دچار پارگی رباط ACL شده بودند نیز این گلاید داخلی را مشاهده کردند.
در انتها به این نکته باید اشاره کنیم که از بیست تحقیق بررسیشده دو تحقیق تأثیر تمرینات توانبخشی را روی تغییرات آرتروکینماتیکی زانوی دارای رباط متقاطع بازسازیشده، بررسی کردند. هوشینو و همکاران تأثیر یک دوره تمرینات دامنه حرکتی و تمرینات قدرتی که به مدت حداکثر نه ماه ادامه پیدا کرد را روی آرتروکینماتیک زانوی بازسازیشده، هنگام دویدن در سراشیبی ارزیابی کردند؛ نتیجه تحقیقات آنها حاکی از این بود که حتی بعد از دوره توانبخشی نیز این افراد در مرحله ضربه پاشنه (هیل استرایک) در هنگام دویدن در سراشیبی به نسبت افراد سالم در مفصل زانو حرکات رول و گلاید بیشتری داشتند [32].
گا اوبو و همکاران نیز برای افرادی که رباط متقاطع قدامی خود را بازسازی کرده بودند یک دوره تمرینات توانبخشی ششمرحلهای شامل تمرینات حمایتی (یک تا هفت روز بعد از عمل)، تمرینات مربوط به تحرک اولیه (هشت تا بیست روز)، حرکات کنترلشده (سه تا شش هفته)، حرکات قدرتی و حس عمقی پیشرفته (هفت تا ده هفته)، تمرینات پلایومتریک و دویدن (یازده تا دوازده هفته) و تمرینات چابکی (سیزده هفته تا شش ماه) را به مدت شش ماه تجویز کردند. نتایج این تحقیق نشان داد متغیرهای کینماتیکی زانوی بازسازی شده علیرغم شرکت در یک برنامه توانبخشی شباهت بیشتری به زانوی آسیبدیده بازسازینشده دارد تا زانوی سالم [46]. در همین راستا هرمان فورماین و همکارانش نیز در تحقیق خود به این نتیجه رسیدهاند، در افرادی که رباط متقاطع خود را بازسازی کردهاند علیرغم شرکت در پروتکل توانبخشی بروز آسیب مجدد در رباط متقاطع قدامی به طور توجهبرانگیزی افزایش یافته است [52]. اینکه چرا بازسازی رباط و متعاقب آن برنامههای توانبخشی نتوانستهاند نتایج مورد انتظار را ایجاد کنند سؤال مهمی است که در مقاله مروری کریستوفر ناجلی و همکارش به آن پرداخته شده است. مقاله مروری آنها با این سؤال شروع میشود که بر اساس ملاحظات زیستشناختی و عملکردی آیا بعد از بازسازی رباط متقاطع قدامی بازگشت به فعالیت ورزشی را باید دو سال به تأخیر انداخت؟ آنها بیان داشتهاند بعد از پارگی رباط و بازسازی آن، چند نکته را باید مورد توجه قرار داد: 1. بعد از بروز آسیب و بازسازی رباط تکثیر سلولهای عروق خونی و عصبی با سرعت کمتری نسبت به مدت زمانی که ورزشکاران به فعالیت بازمیگردند که معمولاًًً بین شش تا دوازده ماه است رخ میدهد [53-56]؛ 2. اغلب اوقات متعاقب آسیب رباط متقاطع قدامی، غضروف و استخوان زیرغضروف نیز به طور توجهبرانگیزی آسیب میبیند [57-60]؛ 3. گیرندههای حسی و میکانیکی سه درصد از حجم بافت رباط را تشکیل میدهند و بین آنها و عضلات اطراف مفصل یک حلقه رفلکسی ایجادشده که به ثبات داینامیک مفصل و حس عمقی آن کمک میکند. زمانی که رباط متقاطع قدامی دچار پارگی میشود، عملکرد حسی کاهش مییابد که علیرغم بازسازی رباط این اختلال عملکرد باقی میماند [61-64]؛ 4. هرچند توانبخشی میتواند بعد از عمل، باعث کاهش افیوژن مفصلی، بهبود دامنه حرکتی و همچنین بهبود قدرت و عملکرد عضله چهارسر شود، ولی به طور خاص ورزشکارانی که رباط خود را بازسازی کردهاند، در کنترل عصبیعضلانی و قدرت اکستنش زانو دارای ویژگیهای مشخصی هستند که تا دو سال بعد از بازسازی به سطح پایه نمیرسند [65-70].
ناجلی و همکارش در انتها به این نتیجه رسیدهاندکه شواهد موجود در ادبیات پیشینه نشان میدهد برای رسیدن به سلامت پایه مفصل بعد از بازسازی رباط و انجام یک دوره توانبخشی در ورزشکاران به حدود دو سال وقت نیاز است و پیشنهاد دادهاند بهتر است، ورزشکارانی که رباط متقاطع قدامی خود را بازسازی کردهاند بهخصوص ورزشکاران جوانتر تا دو سال به فعالیت اصلی خود بازنگردند؛ زیرا بررسی آنها نشان داد تأخیر در بازگشت به فعالیت اصلی تقریباً برای دو سال به طور توجهبرانگیزی بروز آسیب بعدی در این رباط را کاهش میدهد [71].
نتیجهگیری نهایی
به نظر میرسد بیشترین تغییرات آرتروکینماتیکی حاصل از پارگی رباط متقاطع قدامی به ترتیب مربوط به گلاید قدامی در اپیکندیل داخلی بیشتر از اپیکندیل خارجی، گلاید داخلی تیبیا، بیشتر شدن چرخش خارجی یا محدود شدن چرخش داخلی باشد. همچنین مشخص شد بیشترین تغییرات بین دو گروه آسیبدیده و گروه سالم در 15 درجه فلکشن و همچنین نزدیک به اکستنش کامل رخ میدهد. در انتها نتایج تحقیقات بیانگر این موضوع بود که آرتروکینماتیک زانو بعد از بازسازی، با قبل آن مشابهت بیشتری داشت تا با زانوی سالم. همچنین حرکات آرتروکینماتیکی رباط بازسازیشده حتی بعد از یک دوره توانبخشی نیز با زانوی بازسازینشده شباهت بیشتری داشت تا با زانوی سالم. البته باید اضافه کرد که مجموع یافتهها نشان میدهد، برای رسیدن به یک نتیجهگیری دقیقتر به مطالعات با تعداد نمونه بیشتر و روشهای با دقت بالاتر نیاز است.
ملاحظات اخلاقی
پیروی از اصول اخلاق پژوهش
این مقاله از نوع مروری است و مستقیماً از هیچگونه نمونه انسانی یا حیوانی در آن استفاده نشده است.
حامی مالی
این پژوهش هیچگونه کمک مالی از سازمانیهای دولتی، خصوصی و غیرانتفاعی دریافت نکرده است.
مشارکت نویسندگان
روششناسی و نظارت: همه نویسندگان؛ نوشتن پیشنویس و منابع اصلی: مصطفی پاینده، ظاهر محمد عاشور؛ بررسی و ویرایش نهایی: علی اصغر نوراسته.
تعارض منافع
بنابر اظهار نویسندگان این مقاله هیچگونه تعارض منافعی ندارد.
تشکر و قدردانی
بدین وسیله نویسندگان از مسئولین پژوهشی و آموزشی دانشگاه گیلان و دانشکده تربیت بدنی و علوم ورزشی تشکر و قدردانی میکنند.
References
- Kakarlapudi T, Bickerstaff D. Knee instability: Isolated and complex. Br J Sports Med. 2000; 34(5):395-400. [DOI:10.1136/bjsm.34.5.395-a] [PMID] [PMCID]
- Nasseri A, Khataee H, Bryant AL, Lloyd DG, Saxby DJ. Modelling the loading mechanics of anterior cruciate ligament. Comput Methods Programs Biomed. 184:105098. [DOI:10.1016/j.cmpb.2019.105098] [PMID]
- Kiapour AM, Murray MM. Basic science of anterior cruciate ligament injury and repair. Bone Joint Res. 2014; 3(2):20-31. . [DOI:10.1302/2046-3758.32.2000241] [PMID] [PMCID]
- Collins SL, Layde P, Guse CE, Schlotthauer AE, Van Valin SE. The incidence and etiology of anterior cruciate ligament injuries in patients under the age of 18 in the State of Wisconsin. Pediat Therapeut. 2014; 4:196. [DOI:10.4172/2161-0665.1000196]
- Ajuied A, Wong F, Smith C, Norris M, Earnshaw P, Back D, et al. Anterior cruciate ligament injury and radiologic progression of knee osteoarthritis: a systematic review and meta-analysis. Am J Sports Med. 2014; 42(9):2242-52. [DOI:10.1177/0363546513508376] [PMID]
- Kapandi IA. The Physiology of the joints. Edinburgh: Churchhill Livingstone; 1985. https://books.google.com/books?id=k5wTAQAAMAAJ&q
- Frankel VH, Burstein AH, Brooks DB. Biomechanics of internal derangement of the knee: Pathomechanics as determined by analysis oftheinstantcentersofrotation. J Bone Joint Surg Am. 1971; 53:945-962. [DOI:10.2106/00004623-197153050-00010]
- Gerber C, Matter P. Biomechanical analysis of the knee after rupture of the anterior cruciate ligament and it primary repair: An instantcentre analysis of function. J Bone Joint Surg Br. 1983; 65:391-9. [DOI:10.1302/0301-620X.65B4.6874709] [PMID]
- Mitton GR, Ireland WP, Runyon CL. Evaluation of the instantaneous centers of rotation of the stifle before and after repair of torn cruciate ligament by use of the over-the-top technique in dogs. Am J Vet Res. 1991; 52(10):1731-7. [PMID]
- Zatsiorsky VM. Kinematics of human motion. Champaign, Ill: Human Kinetic; 1998. https://books.google.com/books?id=mf4i7G5nXvkC&printsec=frontcover&dq=
- Fu FH, Harner CD, Johnson DL, Miller MD, Woo SL. Biomechanics of knee ligaments: basic concepts and clinical application. Instr Course Lect. 1994; 43:137-48. [PMID]
- Khasian M, LaCour MT, Coomer SC, Bolognesi MP, Komistek RD. In vivo knee kinematics for a cruciate sacrificing total knee arthroplasty having both a symmetrical femoral and tibial component. J Arthroplasty. 2020; 35(6):1712-9. https://www.sciencedirect.com/science/article/abs/pii/S0883540320301273
- Marx RG, Jones EC, Angel M, Wickiewicz TL, Warren RF. Beliefs and attitudes of members of the American Academy of Orthopaedic Surgeons regarding the treatment of anterior cruciate ligament injury. Arthroscopy. 2003; 19(7):762-770. [DOI:10.1016/S0749-8063(03)00398-0]
- Sim JA, Gadikota HR, Li JS, Li G, Gill TJ. Biomechanical evaluation of knee joint laxities and graft forces after anterior cruciate ligament reconstruction by anteromedial portal, outside-in, and transtibial techniques. Am J Sports Med. 2011; 39:2604-10. [DOI:10.1177/0363546511420810] [PMID] [PMCID]
- Herrington L, Alarifi S, Jones R. Patellofemoral joint loads during running at the time of return to sport in elite athletes with acl reconstruction. Am J Sports Med. 2017; 45(12):2812-6. [DOI:10.1177/0363546517716632] [PMID]
- Karanikas K, Arampatzis A, Bruggemann GP. Motor task and muscle strength followed different adaptation patterns after anterior cruciate ligament reconstruction. Eur J Phys Rehabil Med. 2009; 45(1):37-45. https://www.researchgate.net/profile/Adamantios_Arampatzis/publication/23454781_
- Kvist J. Rehabilitation following anterior cruciate ligament injury. Sport Med. 2004; 34(4):269-80. [DOI:10.2165/00007256-200434040-00006] [PMID]
- Noehren B, Abraham A, Curry M, Johnson D, Ireland ML. Evaluation of proximal joint kinematics and muscle strength following ACL reconstruction surgery in female athletes. J Orthop Res. 2014; 32(10):1305-10. [DOI:10.1002/jor.22678] [PMID] [PMCID]
- Pairot-de-Fontenay B, Willy RW, Elias AR, Mizner RL, Dube MO, Roy JS. Running biomechanics in individuals with anterior cruciate ligament reconstruction: A systematic review. Sport Med. 2019; 49(9):1411-24. [DOI:10.1007/s40279-019-01120-x] [PMID]
- Pratt KA, Sigward SM. Knee loading deficits during dynamic tasks in individuals following anterior cruciate ligament reconstruction. J Orthop Sports Phys Ther. 2017; 47(6):411-9. [DOI:10.2519/jospt.2017.6912] [PMID]
- Tashman S, Kolowich P, Collon D, Anderson K, Anderst W. Dynamic function of the ACL-reconstructed knee during running. Clin Orthop Relat Res. 2007; 454:66-73. [DOI:10.1097/BLO.0b013e31802bab3e] [PMID]
- Andersen HN, Dyhre-Poulsen P. The anterior cruciate ligament does play a role in controlling axial rotation in the knee. Knee Surg Sports Traumatol Arthrosc. 1997; 5(3):145-9. [DOI:10.1007/s001670050042] [PMID]
- Ingersoll CD, Grindstaff TL, Pietrosimone BG, Hart JM. Neuromuscular consequences of anterior cruciate ligament injury. Clin Sports Med. 2008; 27(3):383-vii. [DOI:10.1016/j.csm.2008.03.004] [PMID]
- Andriacchi TP, Briant PL, Bevill SL, Koo S. Rotational changes at the knee after ACL injury cause cartilage thinning. Clin Orthop Relat Res. 2006; 442:39-44. [DOI:10.1097/01.blo.0000197079.26600.09] [PMID]
- Chaudhari AMW, Briant PL, Bevill SL, Koo S, Andriacchi TP. Knee kinematics, cartilage morphology, and osteoarthritis after ACL injury. Med Sci Sports Exerc. 2008; 40(2):215-22. [DOI:10.1249/mss.0b013e31815cbb0e] [PMID]
- Barenius B, Ponzer S, Shalabi A, Bujak R, Norlén L, Eriksson K. Increased risk of osteoarthritis after anterior cruciate ligament reconstruction: A 14-year follow-up study of a randomized controlled trial. Am J Sports Med. 2014; 42(5):1049-57. [DOI:10.1177/0363546514526139] [PMID]
- Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998; 52(6):377-84. [DOI:10.1136/jech.52.6.377] [PMID] [PMCID]
- O’Connor SR, Tully MA, Ryan B, Bradley JM, Baxter GD, McDonough SM. Failure of a numerical quality assessment scale to identify potential risk of bias in a systematic review: A comparison study. BMC Res Notes. 2015; 8(1):1-7. https://bmcresnotes.biomedcentral.com/articles/10.1186/s13104-015-1181-1
- Akpinar B, Thorhauer E, Irrgang JJ, Tashman S, Fu FH, Anderst WJ. Alteration of Knee kinematics after anatomic anterior cruciate ligament reconstruction is dependent on associated meniscal injury. Am J Sports Med. 2018; 46(5):1158-65. [DOI:10.1177/0363546517753386] [PMID]
- Andriacchi TP, Dyrby CO. Interactions between kinematics and loading during walking for the normal and ACL deficient knee. J Biomech. 2005; 38(2):293-8. [DOI:10.1016/j.jbiomech.2004.02.010] [PMID]
- Boeth H, Duda GN, Heller MO, Ehrig RM, Doyscher R, Jung T, et al. Anterior cruciate ligament-deficient patients with passive knee joint laxity have a decreased range of anterior-posterior motion during active movements. Am J Sports Med. 2013; 41(5):1051-7. [DOI:10.1177/0363546513480465] [PMID]
- Hoshino Y, Tashman S. Internal tibial rotation during in vivo, dynamic activity induces greater sliding of tibio-femoral joint contact on the medial compartment. Knee Surg Sports Traumatol Arthrosc. 2012; 20(7):1268-75. [DOI:10.1007/s00167-011-1731-6] [PMID]
- Shabani B, Bytyqi D, Lustig S, Cheze L, Bytyqi C, Neyret P. Gait knee kinematics after ACL reconstruction: 3D assessment. Int Orthop. 2015; 39(6):1187-93. [DOI:10.1007/s00264-014-2643-0] [PMID]
- Yang C, Tashiro Y, Lynch A, Fu F, Anderst W. Kinematics and arthrokinematics in the chronic ACL-deficient knee are altered even in the absence of instability symptoms. Knee Surg Sports Traumatol Arthrosc. 2018; 26(5):1406-13. [DOI:10.1007/s00167-017-4780-7] [PMID] [PMCID]
- Yim JH, Seon JK, Kim YK, Jung ST, Shin CS, Yang DH, et al. Anterior translation and rotational stability of anterior cruciate ligament-deficient knees during walking: speed and turning direction. J Orthop Sci. 2015; 20(1):155-62. [DOI:10.1007/s00776-014-0672-6] [PMID]
- Zhang Y, Huang W, Yao Z, Ma L, Lin Z, Wang S, et al. Anterior cruciate ligament injuries alter the kinematics of knees with or without meniscal deficiency. Am J Sports Med. 2016; 44(12):3132-9. [DOI:10.1177/0363546516658026] [PMID]
- Brandsson 1 S, Karlsson J, Eriksson BI, Kärrholm J. Kinematics after tear in the anterior cruciate ligament: Dynamic bilateral radiostereometric studies in 11 patients. Acta Orthop Scand. 2001; 72(4):372-8. [DOI:10.1080/000164701753542032] [PMID]
- Chen K, Yin L, Cheng L, Li C, Chen C, Yang L. In vivo motion of femoral condyles during weight-bearing flexion after anterior cruciate ligament rupture using biplane radiography. J Sports Sci Med. 2013; 12(3):579. [PMCID] [PMID]
- Cone SG, Lambeth EP, Piedrahita JA, Spang JT, Fisher MB. Joint laxity varies in response to partial and complete anterior cruciate ligament injuries throughout skeletal growth. J Biomech. 2020; 101:109636. [DOI:10.1016/j.jbiomech.2020.109636] [PMID]
- DeFrate LE, Papannagari R, Gill TJ, Moses JM, Pathare NP, Li G. The 6 Degrees of Freedom Kinematics of the Knee after Anterior Cruciate Ligament Deficiency: An in Vivo Imaging Analysis. Am J Sports Med. 2006; 34(8):1240-6. [DOI:10.1177/0363546506287299] [PMID]
- Dennis DA, Mahfouz MR, Komistek RD, Hoff W. In vivo determination of normal and anterior cruciate ligament-deficient knee kinematics. J Biomech. 2005; 38(2):241-53. [DOI:10.1016/j.jbiomech.2004.02.042] [PMID]
- Hollman JH, Deusinger RH, Van Dillen LR, Matava MJ. Knee joint movements in subjects without knee pathology and subjects with injured anterior cruciate ligaments. Phys Ther. 2002; 82:960-972. [DOI:10.1093/ptj/82.10.960] [PMID]
- Jonsson H, Kärrholm J, Elmqvist LG. Kinematics of active knee extension after tear of the anterior cruciate ligament. Am J Sports Med. 1989; 17(6):796-802. [DOI:10.1177/036354658901700613] [PMID]
- Abebe ES, Utturkar GM, Taylor DC, Spritzer CE, Kim JP, Moorman CT, et al. The effects of femoral graft placement on in vivo knee kinematics after anterior cruciate ligament reconstruction. J Biomech. 2011; 44(5):924-9. [DOI:10.1016/j.jbiomech.2010.11.028] [PMID] [PMCID]
- Brandsson 2 S, Karlsson J, Swärd L, Kartus J, Eriksson BI, Kärrholm J. Kinematics and laxity of the knee joint after anterior cruciate ligament reconstruction: pre- and postoperative radiostereometric studies. Am J Sports Med. 2002; 30(3):361-7. [DOI:10.1177/03635465020300031001] [PMID]
- Gao B, Zheng N. Alterations in three-dimensional joint kinematics of anterior cruciate ligament-deficient and -reconstructed knees during walking. Clinical Biomechanics. 2010; 25(3):222-9. [DOI:10.1016/j.clinbiomech.2009.11.006] [PMID]
- Kvist J. Sagittal plane knee motion in the ACL-deficient knee during body weight shift exercises on different support surfaces. J Orthop Sports Phys Ther. 2006; 36(12):954-62.[DOI:10.2519/jospt.2006.2290] [PMID]
- Koo S, Kyung BS, Jeong JS, Suh DW, Ahn JH, Wang JH. Dynamic three-dimensional analysis of lachman test for anterior cruciate ligament insufficiency: analysis of anteroposterior motion of the medial and lateral femoral epicondyles. Knee Surg Relat Res. 2015; 27(3):187-93. [DOI:10.5792/ksrr.2015.27.3.187] [PMID] [PMCID]
- Chahla J, Nelson T, Dallo I, Yalamanchili D, Eberlein S, Limpisvasti O, et al. Anterior cruciate ligament repair versus reconstruction: A kinematic analysis. Knee. 2020; 27(2):334-340. [DOI:10.1016/j.knee.2019.10.020][PMID]
- Andriacchi TP, Mundermann A, Smith RL, Alexander EJ, Dyrby CO, Koo S. A framework for the in vivo pathomechanics of osteoarthritis at the knee. Ann Biomed Eng. 2004; 32:447-457. [DOI:10.1023/B:ABME.0000017541.82498.37] [PMID]
- Fairclough JA, Graham GP, Dent CM. Radiological sign of chronic anterior cruciate ligament deficiency. Injury. 1990; 21(6):401-2. [DOI:10.1016/0020-1383(90)90130-M]
- Vermeijden HD, Yang XA, van der List JP, DiFelice GS. Large variation in indications, preferred surgical technique and rehabilitation protocol for primary anterior cruciate ligament repair: A survey among ESSKA members. Knee Surg Sports Traumatol Arthrosc. 2020; 28(11):3613-21. https://link.springer.com/article/10.1007/s00167-020-06011-7
- Amiel D, Kleiner JB, Roux RD, Harwood FL, Akeson WH. The phenomenon of “Ligamentization”: Anterior cruciate ligament reconstruction with autogenous patellar tendon. J Orthop Res. 1986; 4(2):162-72. [DOI:10.1002/jor.1100040204] [PMID]
- Arnoczky SP, Tarvin GB, Marshall JL. Anterior cruciate ligament replacement using patellar tendon. An evaluation of graft revascularization in the dog. J Bone Joint Surg Am. 1982; 64(2):217-24. [DOI:10.2106/00004623-198264020-00011]
- Grindem H, Snyder-Mackler L, Moksnes H, Engebretsen L, Risberg MA. Simple decision rules can reduce reinjury risk by 84% after ACL reconstruction: The Delaware-Oslo ACL cohort study. British J Sports Med. 2016; 50(13):804-8. [DOI:10.1136/bjsports-2016-096031] [PMID] [PMCID]
- Scheffler SU, Unterhauser FN, Weiler A. Graft remodeling and ligamentization after cruciate ligament reconstruction. Knee Surgery, Sports Traumatology, Arthroscopy. 2008; 16(9):834-42. [DOI:10.1007/s00167-008-0560-8] [PMID]
- Abe S, Kurosaka M, Iguchi T, Yoshiya S, Hirohata K. Light and electron microscopic study of remodeling and maturation process in autogenous graft for anterior cruciate ligament reconstruction. Arthroscopy. 1993; 9(4):394-405. [DOI:10.1016/S0749-8063(05)80313-5]
- Claes S, Verdonk P, Forsyth R, Bellemans J. The “Ligamentization” Process in Anterior Cruciate Ligament Reconstruction: What Happens to the Human Graft? A Systematic Review of the Literature. Am J Sports Med. 2011; 39(11):2476-83. [DOI:10.1177/0363546511402662] [PMID]
- Pauzenberger L, Syré S, Schurz M. “Ligamentization” in hamstring tendon grafts after anterior cruciate ligament reconstruction: A systematic review of the literature and a glimpse into the future. Arthroscopy. 2013; 29(10):1712-21. [DOI:10.1016/j.arthro.2013.05.009] [PMID]
- Rougraff B, Shelbourne KD, Gerth PK, Warner J. Arthroscopic and histologic analysis of human patellar tendon autografts used for anterior cruciate ligament reconstruction. Am J Sports Med. 1993; 21(2):277-84. [DOI:10.1177/036354659302100219] [PMID]
- Dyhre-Poulsen P, Krogsgaard MR. Muscular reflexes elicited by electrical stimulation of the anterior cruciate ligament in humans. J Appl Physiol. 2000; 89(6):2191-5. [DOI:10.1152/jappl.2000.89.6.2191] [PMID]
- Krogsgaard MR, Fischer-Rasmussen T, Dyhre-Poulsen P. Absence of sensory function in the reconstructed anterior cruciate ligament. J Electromyogr Kinesiol. 2011; 21(1):82-6. [DOI:10.1016/j.jelekin.2010.09.012] [PMID]
- Ochi M, Iwasa J, Uchio Y, Adachi N, Kawasaki K. Induction of somatosensory evoked potentials by mechanical stimulation in reconstructed anterior cruciate ligaments. J Bone Joint Surg Am. 2002; 84(5):761-6. [DOI:10.1302/0301-620X.84B5.0840761]
- Nyland J, Brosky T, Currier D, Nitz A, Caborn D. Review of the afferent neural system of the knee and its contribution to motor learning. J Orthop Sports Phys The. 1994; 19(1):2-11. [DOI:10.2519/jospt.1994.19.1.2] [PMID]
- Di Stasi SL, Logerstedt D, Gardinier ES, Snyder-Mackler L. Gait patterns differ between acl-reconstructed athletes who pass return-to-sport criteria and those who fail. Am J Sports Med. 2013; 41(6):1310-8. [DOI:10.1177/0363546513482718] [PMID] [PMCID]
- Gokeler A, Benjaminse A, van Eck CF, Webster KE, Schot L, Otten E. Return of normal gait as an outcome measurement in acl reconstructed patients. A systematic review. Int J Sports Phys Ther. 2013; 8(4):441-51. [PMCID] [PMID]
- Hart HF, Culvenor AG, Collins NJ, Ackland DC, Cowan SM, Machotka Z, et al. Knee kinematics and joint moments during gait following anterior cruciate ligament reconstruction: A systematic review and meta-analysis. Br J Sports Med. 2016; 50(10):597-612. [DOI:10.1136/bjsports-2015-094797] [PMID]
- Roewer BD, Di Stasi SL, Snyder-Mackler L. Quadriceps strength and weight acceptance strategies continue to improve two years after anterior cruciate ligament reconstruction. J Biomech. 2011; 44(10):1948-53. [DOI:10.1016/j.jbiomech.2011.04.037] [PMID] [PMCID]
- Stasi SD, Hartigan EH, Snyder-Mackler L. Sex-Specific Gait Adaptations Prior to and up to 6 Months After Anterior Cruciate Ligament Reconstruction. J Orthop Sports Phys. 2015; 45(3):207-14. [DOI:10.2519/jospt.2015.5062] [PMID] [PMCID]
- Xergia SA, Pappas E, Zampeli F, Georgiou S, Georgoulis AD. Asymmetries in Functional Hop Tests, Lower Extremity Kinematics, and Isokinetic Strength Persist 6 to 9 Months Following Anterior Cruciate Ligament Reconstruction. J Orthop Sports Phys. 2013; 43(3):154-62. [DOI:10.2519/jospt.2013.3967] [PMID]
- Nagelli CV, Hewett TE. Should Return to Sport be Delayed Until 2 Years After Anterior Cruciate Ligament Reconstruction? Biological and Functional Considerations. Sports Med (Auckland, NZ). 2017; 47(2):221-32. [DOI:10.1007/s40279-016-0584-z] [PMID] [PMCID]
فهرست منابع
1. T Kakarlapudi, D Bickerstaff. Knee instability: isolated and complex. Br J Sports Med. 2000;34(5): 395-400,. [DOI:10.1136/bjsm.34.5.395-a] [PMID] [PMCID]
2. Nasseri A, Khataee H, Bryant AL, Lloyd DG, Saxby DJ. Modelling the loading mechanics of anterior cruciate ligament. Computer Methods and Programs in Biomedicine. 2020 2020/02/01/;184:105098. [DOI:10.1016/j.cmpb.2019.105098] [PMID]
3. Kiapour AM, Murray MM. Basic science of anterior cruciate ligament injury and repair. Bone Joint Res 2014;3(2):20-31. . [DOI:10.1302/2046-3758.32.2000241] [PMID] [PMCID]
4. Collins SL, Layde P, Guse CE, Schlotthauer AE, Van Valin SE. The Incidence and Etiology of Anterior Cruciate Ligament Injuries in Patients under the Age of 18 in the State of Wisconsin,. Pediat Therapeut 2014;4: 196. doi:10.4172/2161-0665.1000196. [DOI:10.4172/2161-0665.1000196]
5. Ajuied A, Wong F, Smith C, Norris M, Earnshaw P, Back D, et al. Anterior cruciate ligament injury and radiologic progression of knee osteoarthritis: a systematic review and meta-analysis. Am J Sports Med. 2014;42(9):2242-52. PubMed PMID: 24214929. Epub 11/08. eng. [DOI:10.1177/0363546513508376] [PMID]
6. Kapandi IA. The Physiology of the joints,. Edinburgh: Churchhill Livingstone,. 1985;vol. 2, Lower limb 5th ed.
7. Frankel VH, Burstein AH, Brooks DB. Biomechanics of internal derangement of the knee: pathomechanics as determined by analysis oftheinstantcentersofrotation. JBoneJointSurgAm. 1971;53:945-962. [DOI:10.2106/00004623-197153050-00010]
8. Gerber C, Matter P. Biomechanical analysis of the knee after rupture of the anterior cruciate ligament and it primary repair: an instantcentre analysis of function. J Bone Joint Surg Br,. 1983;65:391-399. [DOI:10.1302/0301-620X.65B4.6874709] [PMID]
9. Mitton GR, Ireland WP, Runyon CL. Evaluation of the instantaneous centers of rotation of the stifle before and after repair of torn cruciate ligament by use of the over-the-top technique in dogs. Am J Vet Res,. 1991;52:1731-1737.
10. Zatsiorsky VM. Kinematics of Human Motion,. Champaign, Ill: Human Kinetic,. 1998, .
11. Fu FH, Harner CD, Johnson DL, Miller MD, Woo SL. Biomechanics of knee ligaments: basic concepts and clinical application. Instr Course Lect. 1994;43:137-48. PubMed PMID: 9097144. eng.
12. Khasian M, LaCour MT, Coomer SC, Bolognesi M, Komistek RD. In Vivo Knee Kinematics for a Cruciate Sacrificing TKA Having Both a Symmetrical Femoral and Tibial Component. The Journal of Arthroplasty. 2020 2020/02/08/;doi.org/10.1016/j.arth.2020.02.004.
13. Marx RG, Jones EC, Angel M, Wickiewicz TL, RF. W. Beliefs and attitudes of members of the American Academy of Orthopaedic Surgeons regarding the treatment of anterior cruciate ligament injury,. Arthroscopy. 2003;19:762-770. [PubMed: 12966385]. [DOI:10.1016/S0749-8063(03)00398-0]
14. Sim JA, Gadikota HR, Li JS, Li G, Gill TJ. Biomechanical evaluation of knee joint laxities and graft forces after anterior cruciate ligament reconstruction by anteromedial portal, outside-in, and transtibial techniques. . Am J Sports Med,. 2011; 39:2604-2610. [PubMed: 21908717],. [DOI:10.1177/0363546511420810] [PMID] [PMCID]
15. Herrington L, Alarifi S, Jones R. Patellofemoral Joint Loads During Running at the Time of Return to Sport in Elite Athletes With ACL Reconstruction. Am J Sports Med. 2017 Oct;45(12):2812-6. PubMed PMID: 28749699. Epub 2017/07/28. eng. [DOI:10.1177/0363546517716632] [PMID]
16. Karanikas K, Arampatzis A, Brüggemann GP. Motor task and muscle strength followed different adaptation patterns after anterior cruciate ligament reconstruction. European journal of physical and rehabilitation medicine. 2009 Mar;45(1):37-45. PubMed PMID: 18987563. Epub 2008/11/07. eng.
17. Kvist J. Rehabilitation following anterior cruciate ligament injury: current recommendations for sports participation. Sports medicine (Auckland, NZ). 2004;34(4):269-80. PubMed PMID: 15049718. Epub 2004/03/31. eng. [DOI:10.2165/00007256-200434040-00006] [PMID]
18. Noehren B, Abraham A, Curry M, Johnson D, Ireland ML. Evaluation of proximal joint kinematics and muscle strength following ACL reconstruction surgery in female athletes. Journal of orthopaedic research : official publication of the Orthopaedic Research Society. 2014 Oct;32(10):1305-10. PubMed PMID: 25044305. Pubmed Central PMCID: PMC4314615. Epub 2014/07/22. eng. [DOI:10.1002/jor.22678] [PMID] [PMCID]
19. Pairot-de-Fontenay B, Willy RW, Elias ARC, Mizner RL, Dubé M-O, Roy J-S. Running Biomechanics in Individuals with Anterior Cruciate Ligament Reconstruction: A Systematic Review. Sports Medicine. 2019; 49(9):1411-24. [DOI:10.1007/s40279-019-01120-x] [PMID]
20. Pratt KA, Sigward SM. Knee Loading Deficits During Dynamic Tasks in Individuals Following Anterior Cruciate Ligament Reconstruction. J Orthop Sports Phys Ther. 2017 Jun;47(6):411-9. PubMed PMID: 28499343. Epub 2017/05/14. eng. [DOI:10.2519/jospt.2017.6912] [PMID]
21. Tashman S, Kolowich P, Collon D, Anderson K, Anderst W. Dynamic function of the ACL-reconstructed knee during running. Clin Orthop Relat Res. 2007 Jan;454:66-73. PubMed PMID: 17091011. Epub 2006/11/09. eng. [DOI:10.1097/BLO.0b013e31802bab3e] [PMID]
22. Andersen HN, Dyhre-Poulsen P. The anterior cruciate ligament does play a role in controlling axial rotation in the knee. Knee Surg Sports Traumatol Arthrosc. 1997;5(3):145-9. PubMed PMID: 9335025. eng. [DOI:10.1007/s001670050042] [PMID]
23. Ingersoll CD, Grindstaff TL, Pietrosimone BG, Hart JM. Neuromuscular consequences of anterior cruciate ligament injury. Clin Sports Med. 2008;27(3):383-vii. PubMed PMID: 18503874. eng. [DOI:10.1016/j.csm.2008.03.004] [PMID]
24. Andriacchi TP, Briant PL, Bevill SL, Koo S. Rotational changes at the knee after ACL injury cause cartilage thinning. Clin Orthop Relat Res. 2006;442:39-44. PubMed PMID: 16394737. eng. [DOI:10.1097/01.blo.0000197079.26600.09] [PMID]
25. Chaudhari AMW, Briant PL, Bevill SL, Koo S, Andriacchi TP. Knee kinematics, cartilage morphology, and osteoarthritis after ACL injury. Med Sci Sports Exerc. 2008;40(2):215-22. PubMed PMID: 18202582. eng. [DOI:10.1249/mss.0b013e31815cbb0e] [PMID]
26. Barenius B, Ponzer S, Shalabi A, Bujak R, Norlén L, Eriksson K. Increased Risk of Osteoarthritis After Anterior Cruciate Ligament Reconstruction: A 14-Year Follow-up Study of a Randomized Controlled Trial. Am J Sports Med. 2014 2014/05/01;42(5):1049-57. [DOI:10.1177/0363546514526139] [PMID]
27. Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. Journal of epidemiology and community health. 1998 Jun;52(6):377-84. PubMed PMID: 9764259. Pubmed Central PMCID: PMC1756728. Epub 1998/10/09. eng. [DOI:10.1136/jech.52.6.377] [PMID] [PMCID]
28. O'Connor SR, Tully MA, Ryan B, Bradley JM, Baxter GD, McDonough SM. Failure of a numerical quality assessment scale to identify potential risk of bias in a systematic review: a comparison study. BMC research notes. 2015 Jun 6;8:224. PubMed PMID: 26048813. Pubmed Central PMCID: PMC4467625. Epub 2015/06/07. eng.
29. Akpinar B, Thorhauer E, Irrgang JJ, Tashman S, Fu FH, Anderst WJ. Alteration of Knee Kinematics After Anatomic Anterior Cruciate Ligament Reconstruction Is Dependent on Associated Meniscal Injury. Am J Sports Med. 2018 2018/04/01;46(5):1158-65. [DOI:10.1177/0363546517753386] [PMID]
30. Andriacchi TP, Dyrby CO. Interactions between kinematics and loading during walking for the normal and ACL deficient knee. J Biomech. 2005;38(2):293-8. PubMed PMID: 15598456. eng. [DOI:10.1016/j.jbiomech.2004.02.010] [PMID]
31. Boeth H, Duda GN, Heller MO, Ehrig RM, Doyscher R, Jung T, et al. Anterior Cruciate Ligament-Deficient Patients With Passive Knee Joint Laxity Have a Decreased Range of Anterior-Posterior Motion During Active Movements. Am J Sports Med. 2013;41(5):1051-7. PubMed PMID: 23492824. [DOI:10.1177/0363546513480465] [PMID]
32. Hoshino Y, Tashman S. Internal tibial rotation during in vivo, dynamic activity induces greater sliding of tibio-femoral joint contact on the medial compartment. Knee Surg Sports Traumatol Arthrosc. 2012 2012/07//;20(7):1268-75. PubMed PMID: 22041716. eng. [DOI:10.1007/s00167-011-1731-6] [PMID]
33. Shabani B, Bytyqi D, Lustig S, Cheze L, Bytyqi C, Neyret P. Gait knee kinematics after ACL reconstruction: 3D assessment. Int Orthop. 2015;39(6):1187-93. PubMed PMID: 25549917. Epub 12/31. eng. [DOI:10.1007/s00264-014-2643-0] [PMID]
34. Yang C, Tashiro Y, Lynch A, Fu F, Anderst W. Kinematics and arthrokinematics in the chronic ACL-deficient knee are altered even in the absence of instability symptoms. Knee Surg Sports Traumatol Arthrosc. 2018;26(5):1406-13. PubMed PMID: 29124285. Epub 11/09. eng. [DOI:10.1007/s00167-017-4780-7] [PMID] [PMCID]
35. Yim JH, Seon JK, Kim YK, Jung ST, Shin CS, Yang DH, et al. Anterior translation and rotational stability of anterior cruciate ligament-deficient knees during walking: speed and turning direction. Journal of Orthopaedic Science. 2015 2015/01/01;20(1):155-62. [DOI:10.1007/s00776-014-0672-6] [PMID]
36. Zhang Y, Huang W, Yao Z, Ma L, Lin Z, Wang S, et al. Anterior Cruciate Ligament Injuries Alter the Kinematics of Knees With or Without Meniscal Deficiency. Am J Sports Med. 2016;44(12):3132-9. PubMed PMID: 27511793. Epub 08/10. eng. [DOI:10.1177/0363546516658026] [PMID]
37. Brandsson S, Karlsson J, Eriksson B, Kärrholm J, . Kinematics after tear in the anterior cruciate ligament: dynamic bilateral radiostereometric studies in 11 patients. Acta orthopaedica Scandinavica,. (2001);72 4, 372-8 . [DOI:10.1080/000164701753542032] [PMID]
38. Chen K, Yin L, Cheng L, Li C, Chen C, Yang L. In vivo motion of femoral condyles during weight-bearing flexion after anterior cruciate ligament rupture using biplane radiography. J Sports Sci Med. 2013;12(3):579-87. PubMed PMID: 24149168. eng.
39. Cone SG, Lambeth EP, Piedrahita JA, Spang JT, Fisher MB. Joint laxity varies in response to partial and complete anterior cruciate ligament injuries throughout skeletal growth. J Biomech. 2020 2020/03/05/;101:109636. [DOI:10.1016/j.jbiomech.2020.109636] [PMID]
40. DeFrate LE, Papannagari R, Gill TJ, Moses JM, Pathare NP, Li G. The 6 Degrees of Freedom Kinematics of the Knee after Anterior Cruciate Ligament Deficiency: An in Vivo Imaging Analysis. Am J Sports Med. 2006 2006/08/01;34(8):1240-6. [DOI:10.1177/0363546506287299] [PMID]
41. Dennis DA, Mahfouz MR, Komistek RD, Hoff W. In vivo determination of normal and anterior cruciate ligament-deficient knee kinematics. J Biomech. 2005;38(2):241-53. PubMed PMID: 15598450. eng. [DOI:10.1016/j.jbiomech.2004.02.042] [PMID]
42. Hollman JH, Deusinger RH, Van Dillen LR, Matava MJ. Knee joint movements in subjects without knee pathology and subjects with injured anterior cruciate ligaments. Phys Ther,. 2002, ;82:960-972. [DOI:10.1093/ptj/82.10.960] [PMID]
43. Jonsson H, Kärrholm J, Elmqvist LG. Kinematics of active knee extension after tear of the anterior cruciate ligament. Am J Sports Med. 1989 Nov-Dec;17(6):796-802. PubMed PMID: 2624292. eng. [DOI:10.1177/036354658901700613] [PMID]
44. Abebe ES, Utturkar GM, Taylor DC, Spritzer CE, Kim JP, Moorman CT, 3rd, et al. The effects of femoral graft placement on in vivo knee kinematics after anterior cruciate ligament reconstruction. J Biomech. 2011;44(5):924-9. PubMed PMID: 21227425. Epub 01/11. eng. [DOI:10.1016/j.jbiomech.2010.11.028] [PMID] [PMCID]
45. Brandsson S, Karlsson J, Swärd L, Kartus J, Eriksson BI, Kärrholm J. Kinematics and laxity of the knee joint after anterior cruciate ligament reconstruction: pre- and postoperative radiostereometric studies. Am J Sports Med. 2002 May-Jun;30(3):361-7. PubMed PMID: 12016076. eng. [DOI:10.1177/03635465020300031001] [PMID]
46. Gao B, Zheng N. Alterations in three-dimensional joint kinematics of anterior cruciate ligament-deficient and -reconstructed knees during walking. Clinical Biomechanics. 2010 2010/03/01/;25(3):222-9. [DOI:10.1016/j.clinbiomech.2009.11.006] [PMID]
47. Kvist J. Sagittal plane knee motion in the ACL-deficient knee during body weight shift exercises on different support surfaces. J Orthop Sports Phys Ther. 2006;36(12):954-62. PubMed PMID: 17193873. eng. [DOI:10.2519/jospt.2006.2290] [PMID]
48. Koo S, Kyung BS, Jeong JS, Suh DW, Ahn JH, Wang JH. Dynamic Three-Dimensional Analysis of Lachman Test for Anterior Cruciate Ligament Insufficiency: Analysis of Anteroposterior Motion of the Medial and Lateral Femoral Epicondyles. Knee Surg Relat Res. 2015;27(3):187-93. PubMed PMID: 26389073. Epub 09/01. eng. [DOI:10.5792/ksrr.2015.27.3.187] [PMID] [PMCID]
49. Chahla J, Nelson T, Dallo I, Yalamanchili D, Eberlein S, Limpisvasti O, et al. Anterior cruciate ligament repair versus reconstruction: A kinematic analysis. The Knee. 2019 2019/12/05/.
50. Andriacchi TP, Mundermann A, Smith RL, Alexander EJ, Dyrby CO, Koo S. A framework for the in vivo pathomechanics of osteoarthritis at the knee. Ann Biomed Eng 2004;32:447-457. [PubMed: 15095819]. [DOI:10.1023/B:ABME.0000017541.82498.37] [PMID]
51. Fairclough JA, Graham GP, Dent CM. Radiological sign of chronic anterior cruciate ligament deficiency. Injury. 1990 1990/11/01/;21(6):401-2. [DOI:10.1016/0020-1383(90)90130-M]
52. Vermeijden HD, Yang XA, van der List JP, DiFelice GS. Large variation in indications, preferred surgical technique and rehabilitation protocol for primary anterior cruciate ligament repair: a survey among ESSKA members. Knee Surg Sports Traumatol Arthrosc. 2020 Apr 23. PubMed PMID: 32328697. Epub 2020/04/25. eng.
53. Amiel D, Kleiner JB, Roux RD, Harwood FL, Akeson WH. The phenomenon of "Ligamentization": Anterior cruciate ligament reconstruction with autogenous patellar tendon. Journal of Orthopaedic Research. 1986;4(2):162-72. [DOI:10.1002/jor.1100040204] [PMID]
54. Arnoczky SP, Tarvin GB, Marshall JL. Anterior cruciate ligament replacement using patellar tendon. An evaluation of graft revascularization in the dog. The Journal of bone and joint surgery American volume. 1982 Feb;64(2):217-24. PubMed PMID: 7056776. Epub 1982/02/01. eng. [DOI:10.2106/00004623-198264020-00011]
55. Grindem H, Snyder-Mackler L, Moksnes H, Engebretsen L, Risberg MA. Simple decision rules can reduce reinjury risk by 84% after ACL reconstruction: the Delaware-Oslo ACL cohort study. British Journal of Sports Medicine. 2016;50(13):804-8. [DOI:10.1136/bjsports-2016-096031] [PMID] [PMCID]
56. Scheffler SU, Unterhauser FN, Weiler A. Graft remodeling and ligamentization after cruciate ligament reconstruction. Knee Surgery, Sports Traumatology, Arthroscopy. 2008 2008/09/01;16(9):834-42. [DOI:10.1007/s00167-008-0560-8] [PMID]
57. Abe S, Kurosaka M, Iguchi T, Yoshiya S, Hirohata K. Light and electron microscopic study of remodeling and maturation process in autogenous graft for anterior cruciate ligament reconstruction. Arthroscopy: The Journal of Arthroscopic & Related Surgery. 1993 1993/08/01/;9(4):394-405. [DOI:10.1016/S0749-8063(05)80313-5]
58. Claes S, Verdonk P, Forsyth R, Bellemans J. The "Ligamentization" Process in Anterior Cruciate Ligament Reconstruction:What Happens to the Human Graft? A Systematic Review of the Literature. Am J Sports Med. 2011;39(11):2476-83. PubMed PMID: 21515806. [DOI:10.1177/0363546511402662] [PMID]
59. Pauzenberger L, Syré S, Schurz M. "Ligamentization" in Hamstring Tendon Grafts After Anterior Cruciate Ligament Reconstruction: A Systematic Review of the Literature and a Glimpse Into the Future. Arthroscopy: The Journal of Arthroscopic & Related Surgery. 2013 2013/10/01/;29(10):1712-21. [DOI:10.1016/j.arthro.2013.05.009] [PMID]
60. Rougraff B, Shelbourne KD, Gerth PK, Warner J. Arthroscopic and histologic analysis of human patellar tendon autografts used for anterior cruciate ligament reconstruction. Am J Sports Med. 1993;21(2):277-84. PubMed PMID: 8465925. [DOI:10.1177/036354659302100219] [PMID]
61. Dyhre-Poulsen P, Krogsgaard MR. Muscular reflexes elicited by electrical stimulation of the anterior cruciate ligament in humans. Journal of Applied Physiology. 2000;89(6):2191-5. PubMed PMID: 11090567. [DOI:10.1152/jappl.2000.89.6.2191] [PMID]
62. Krogsgaard MR, Fischer-Rasmussen T, Dyhre-Poulsen P. Absence of sensory function in the reconstructed anterior cruciate ligament. Journal of Electromyography and Kinesiology. 2011 2011/02/01/;21(1):82-6. [DOI:10.1016/j.jelekin.2010.09.012] [PMID]
63. M. O, J. I, Y. U, N. A, K. K. Induction of somatosensory evoked potentials by mechanical stimulation in reconstructed anterior cruciate ligaments. The Journal of Bone and Joint Surgery British volume. 2002;84-B(5):761-6. [DOI:10.1302/0301-620X.84B5.0840761]
64. Nyland J, Brosky T, Currier D, Nitz A, Caborn D. Review of the Afferent Neural System of the Knee and Its Contribution to Motor Learning. Journal of Orthopaedic & Sports Physical Therapy. 1994;19(1):2-11. PubMed PMID: 8156059. [DOI:10.2519/jospt.1994.19.1.2] [PMID]
65. Di Stasi SL, Logerstedt D, Gardinier ES, Snyder-Mackler L. Gait Patterns Differ Between ACL-Reconstructed Athletes Who Pass Return-to-Sport Criteria and Those Who Fail. Am J Sports Med. 2013;41(6):1310-8. PubMed PMID: 23562809. [DOI:10.1177/0363546513482718] [PMID] [PMCID]
66. Gokeler A, Benjaminse A, van Eck CF, Webster KE, Schot L, Otten E. Return of normal gait as an outcome measurement in acl reconstructed patients. A systematic review. Int J Sports Phys Ther. 2013;8(4):441-51. PubMed PMID: 24175130. eng.
67. Hart HF, Culvenor AG, Collins NJ, Ackland DC, Cowan SM, Machotka Z, et al. Knee kinematics and joint moments during gait following anterior cruciate ligament reconstruction: a systematic review and meta-analysis. British Journal of Sports Medicine. 2016;50(10):597-612. [DOI:10.1136/bjsports-2015-094797] [PMID]
68. Roewer BD, Di Stasi SL, Snyder-Mackler L. Quadriceps strength and weight acceptance strategies continue to improve two years after anterior cruciate ligament reconstruction. J Biomech. 2011 2011/07/07/;44(10):1948-53. [DOI:10.1016/j.jbiomech.2011.04.037] [PMID] [PMCID]
69. Stasi SD, Hartigan EH, Snyder-Mackler L. Sex-Specific Gait Adaptations Prior to and up to 6 Months After Anterior Cruciate Ligament Reconstruction. Journal of Orthopaedic & Sports Physical Therapy. 2015;45(3):207-14. PubMed PMID: 25627155. [DOI:10.2519/jospt.2015.5062] [PMID] [PMCID]
70. Xergia SA, Pappas E, Zampeli F, Georgiou S, Georgoulis AD. Asymmetries in Functional Hop Tests, Lower Extremity Kinematics, and Isokinetic Strength Persist 6 to 9 Months Following Anterior Cruciate Ligament Reconstruction. Journal of Orthopaedic & Sports Physical Therapy. 2013;43(3):154-62. PubMed PMID: 23322072. [DOI:10.2519/jospt.2013.3967] [PMID]
71. Nagelli CV, Hewett TE. Should Return to Sport be Delayed Until 2 Years After Anterior Cruciate Ligament Reconstruction? Biological and Functional Considerations. Sports medicine (Auckland, NZ). 2017;47(2):221-32. PubMed PMID: 27402457. eng. [DOI:10.1007/s40279-016-0584-z] [PMID] [PMCID]
| بازنشر اطلاعات | |
 |
این مقاله تحت شرایط Creative Commons Attribution-NonCommercial 4.0 International License قابل بازنشر است. |

تماس با ما
فصلنامه بیومکانیک ورزشی
همدان،شهرک مدنی، بلوار امام خمینی(ره)، بلوار پروفسور موسیوند، مجتمع دانشگاه آزاد اسلامی واحد همدان، معاونت پژوهش و فناوری، دفتر مجلات علمی
صندوق پستی: 734
تلفن دفتر نشریه: 08134494042
وبسایت: http://biomechanics.iauh.ac.ir
ایمیل: sportbiomechanics@iauh.ac.ir