

Volume 10, Issue 4 (1-2025)
J Sport Biomech 2025, 10(4): 262-275 |
Back to browse issues page



![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Aghamohammadi F, Jalalvand A. The Effect of Different Walking Strategies (Normal, Toe-Out, and Toe-In) on Maximum Force and Plantar Pressure in Ten Regions of the Foot. J Sport Biomech 2025; 10 (4) :262-275
URL: http://biomechanics.iauh.ac.ir/article-1-360-en.html
URL: http://biomechanics.iauh.ac.ir/article-1-360-en.html



1- Department of Sport Biomechanics, Hamedan Branch, Islamic Azad University, Hamedan, Iran.
Full-Text [PDF 1694 kb]
(972 Downloads)
| Abstract (HTML) (2989 Views)
Full-Text: (1195 Views)
Extended Abstract
1. Introduction
A wide range of interventions and strategies are considered for individuals with osteoarthritis (6). Recent research indicates that modifying gait patterns can effectively reduce knee adduction torque in patients with knee osteoarthritis (7). Studies have shown that rotating the foot outward (toe-out) or inward (toe-in) during gait decreases both the initial and secondary peaks of knee adduction torque, which is one of the therapeutic goals for these patients (8). However, research on the most effective gait pattern for these patients remains limited and inconclusive. The use of modified gait can help adjust and distribute plantar pressure, reduce pain, and improve muscle function in individuals with various lower limb pathologies, such as knee osteoarthritis, flat feet, and high arches. In patients with joint mobility limitations, ground reaction forces (GRFs) are not distributed normally across a larger area of the foot, leading to increased pressure in specific plantar regions during gait. For instance, in diabetic patients, repetitive pressure on a localized area of the foot during walking can lead to callus formation and, ultimately, foot ulcers. Additionally, during the push-off phase, ineffective force transmission from the ankle to the upper body results in prolonged pressure duration, increased impact, and, consequently, forefoot ulcers (9). These findings highlight the significance of modified gait patterns in redistributing forces and mitigating excessive pressure on specific foot regions. Despite the potential benefits, research on the most effective walking strategies for target populations remains limited. Therefore, the present study investigates the effects of different gait strategies (normal, toe-out, and toe-in) on plantar pressure variables. This research may provide new insights into pain reduction and biomechanical correction in various lower limb pathologies using non-invasive methods.
2. Methods
The statistical population of this study comprised healthy male university students aged 18 to 25 years. The sample size was determined using G*Power software, estimating 21 participants for the mixed-design analysis of variance (10). To record plantar pressure variables and load distribution across ten foot regions, the RsScan International footscan device was used, with a sampling frequency set at 253 Hz. Participants performed gait trials under three conditions—normal walking, toe-out walking, and toe-in walking—while barefoot. Each walking strategy was tested in three trials. Data analysis was conducted using repeated measures multivariate analysis of variance (MANOVA) in SPSS software (p ≤ 0.05). The Bonferroni post-hoc test was applied for pairwise comparisons.
3. Results
When walking with a toe-in pattern compared to normal walking, the maximum plantar force in the big toe, first and second metatarsals, and medial heel significantly decreases (p < 0.05), while the maximum plantar force in the fourth and fifth metatarsals and the midfoot region significantly increases (p < 0.05). When walking with a toe-out pattern compared to normal walking, the maximum plantar force in the first metatarsal significantly increases (p < 0.05), while it significantly decreases in the third and fourth metatarsals (p < 0.05). Walking with a toe-out pattern compared to a toe-in pattern significantly increases the maximum plantar force in the first metatarsal (p < 0.05) but significantly decreases it in the third and fourth metatarsals (p < 0.05). Walking with a toe-in pattern compared to a toe-out pattern significantly decreases the maximum plantar force in the first metatarsal (p < 0.05) and significantly increases it in the fifth metatarsal (p < 0.05).
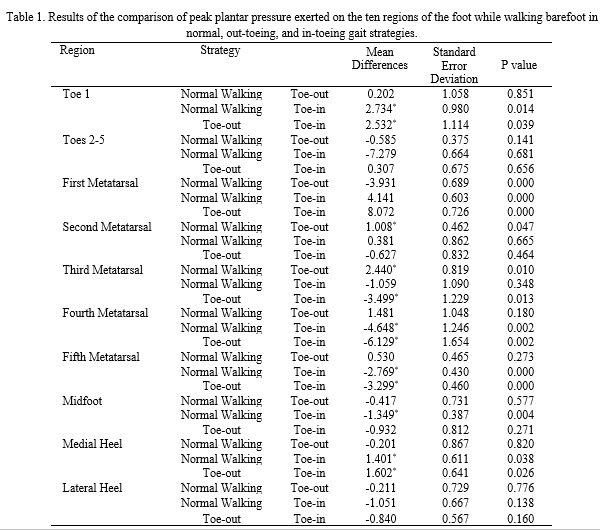
When walking with a toe-in pattern compared to normal and toe-out walking, the maximum plantar pressure in the big toe and medial heel significantly decreases (p < 0.05), while the maximum plantar pressure in the fourth and fifth metatarsals significantly increases (p < 0.05). When walking with a toe-in pattern compared to normal walking, the maximum plantar pressure in the first metatarsal significantly decreases (p < 0.05), while it significantly increases in the midfoot region (p < 0.05). When walking with a toe-out pattern compared to normal walking, the maximum plantar pressure in the first metatarsal significantly increases (p < 0.05), while it significantly decreases in the second and third metatarsals (p < 0.05). When walking with a toe-out pattern compared to a toe-in pattern, the maximum plantar pressure in the first metatarsal significantly increases (p < 0.05), while it significantly decreases in the third metatarsal (p < 0.05) (Table 1).
4. Conclusion
Adopting a toe-in gait strategy can be an optimal approach in rehabilitation and exercise therapy for individuals with patellofemoral pain syndrome (12), as it reduces the forces exerted on the first and second metatarsals. Conversely, adopting a toe-out gait strategy is a risk factor and may exacerbate this condition. Stress fractures in bones are associated with increased loading in various regions of the foot (14). Some research findings indicate that individuals with flat feet experience greater loading in the medial region of the foot (5). Therefore, individuals with flat feet who adopt a toe-out gait strategy are at a potential risk of developing stress fractures in the second to fifth toes, as well as the first and second metatarsals. Individuals with high arches experience greater overall stiffness in the lower leg and a higher external loading rate compared to those with flat feet during activity (15). Since the toe-out gait pattern reduces the force exerted on the lateral bones of the foot, it can be considered a force-modifying strategy for individuals with high arches and may be incorporated into their rehabilitation approaches. On the other hand, high arches can lead to issues in the hip and knee joints and are a risk factor for lateral ankle sprains (17). Therefore, the toe-out gait pattern may help prevent injuries to the lower limb joints, particularly lateral ankle sprains, which are highly prevalent. Increased loading in the medial region of the foot is a risk factor for inversion ankle sprains. Thus, immediately after inducing fatigue, the toe-out gait strategy can serve as a force-distribution-modifying strategy for individuals with high arches (18).
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be addressed in this research.
Funding
This research did not receive any financial support from government, private, or non-profit organizations.
Authors' contributions
All authors contributed equally to preparing the article.
Conflicts of interest
The authors declare that there are no conflicts of interest associated with this article.
A wide range of interventions and strategies are considered for individuals with osteoarthritis (6). Recent research indicates that modifying gait patterns can effectively reduce knee adduction torque in patients with knee osteoarthritis (7). Studies have shown that rotating the foot outward (toe-out) or inward (toe-in) during gait decreases both the initial and secondary peaks of knee adduction torque, which is one of the therapeutic goals for these patients (8). However, research on the most effective gait pattern for these patients remains limited and inconclusive. The use of modified gait can help adjust and distribute plantar pressure, reduce pain, and improve muscle function in individuals with various lower limb pathologies, such as knee osteoarthritis, flat feet, and high arches. In patients with joint mobility limitations, ground reaction forces (GRFs) are not distributed normally across a larger area of the foot, leading to increased pressure in specific plantar regions during gait. For instance, in diabetic patients, repetitive pressure on a localized area of the foot during walking can lead to callus formation and, ultimately, foot ulcers. Additionally, during the push-off phase, ineffective force transmission from the ankle to the upper body results in prolonged pressure duration, increased impact, and, consequently, forefoot ulcers (9). These findings highlight the significance of modified gait patterns in redistributing forces and mitigating excessive pressure on specific foot regions. Despite the potential benefits, research on the most effective walking strategies for target populations remains limited. Therefore, the present study investigates the effects of different gait strategies (normal, toe-out, and toe-in) on plantar pressure variables. This research may provide new insights into pain reduction and biomechanical correction in various lower limb pathologies using non-invasive methods.
2. Methods
The statistical population of this study comprised healthy male university students aged 18 to 25 years. The sample size was determined using G*Power software, estimating 21 participants for the mixed-design analysis of variance (10). To record plantar pressure variables and load distribution across ten foot regions, the RsScan International footscan device was used, with a sampling frequency set at 253 Hz. Participants performed gait trials under three conditions—normal walking, toe-out walking, and toe-in walking—while barefoot. Each walking strategy was tested in three trials. Data analysis was conducted using repeated measures multivariate analysis of variance (MANOVA) in SPSS software (p ≤ 0.05). The Bonferroni post-hoc test was applied for pairwise comparisons.
3. Results
When walking with a toe-in pattern compared to normal walking, the maximum plantar force in the big toe, first and second metatarsals, and medial heel significantly decreases (p < 0.05), while the maximum plantar force in the fourth and fifth metatarsals and the midfoot region significantly increases (p < 0.05). When walking with a toe-out pattern compared to normal walking, the maximum plantar force in the first metatarsal significantly increases (p < 0.05), while it significantly decreases in the third and fourth metatarsals (p < 0.05). Walking with a toe-out pattern compared to a toe-in pattern significantly increases the maximum plantar force in the first metatarsal (p < 0.05) but significantly decreases it in the third and fourth metatarsals (p < 0.05). Walking with a toe-in pattern compared to a toe-out pattern significantly decreases the maximum plantar force in the first metatarsal (p < 0.05) and significantly increases it in the fifth metatarsal (p < 0.05).
When walking with a toe-in pattern compared to normal and toe-out walking, the maximum plantar pressure in the big toe and medial heel significantly decreases (p < 0.05), while the maximum plantar pressure in the fourth and fifth metatarsals significantly increases (p < 0.05). When walking with a toe-in pattern compared to normal walking, the maximum plantar pressure in the first metatarsal significantly decreases (p < 0.05), while it significantly increases in the midfoot region (p < 0.05). When walking with a toe-out pattern compared to normal walking, the maximum plantar pressure in the first metatarsal significantly increases (p < 0.05), while it significantly decreases in the second and third metatarsals (p < 0.05). When walking with a toe-out pattern compared to a toe-in pattern, the maximum plantar pressure in the first metatarsal significantly increases (p < 0.05), while it significantly decreases in the third metatarsal (p < 0.05) (Table 1).
4. Conclusion
Adopting a toe-in gait strategy can be an optimal approach in rehabilitation and exercise therapy for individuals with patellofemoral pain syndrome (12), as it reduces the forces exerted on the first and second metatarsals. Conversely, adopting a toe-out gait strategy is a risk factor and may exacerbate this condition. Stress fractures in bones are associated with increased loading in various regions of the foot (14). Some research findings indicate that individuals with flat feet experience greater loading in the medial region of the foot (5). Therefore, individuals with flat feet who adopt a toe-out gait strategy are at a potential risk of developing stress fractures in the second to fifth toes, as well as the first and second metatarsals. Individuals with high arches experience greater overall stiffness in the lower leg and a higher external loading rate compared to those with flat feet during activity (15). Since the toe-out gait pattern reduces the force exerted on the lateral bones of the foot, it can be considered a force-modifying strategy for individuals with high arches and may be incorporated into their rehabilitation approaches. On the other hand, high arches can lead to issues in the hip and knee joints and are a risk factor for lateral ankle sprains (17). Therefore, the toe-out gait pattern may help prevent injuries to the lower limb joints, particularly lateral ankle sprains, which are highly prevalent. Increased loading in the medial region of the foot is a risk factor for inversion ankle sprains. Thus, immediately after inducing fatigue, the toe-out gait strategy can serve as a force-distribution-modifying strategy for individuals with high arches (18).
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be addressed in this research.
Funding
This research did not receive any financial support from government, private, or non-profit organizations.
Authors' contributions
All authors contributed equally to preparing the article.
Conflicts of interest
The authors declare that there are no conflicts of interest associated with this article.
Type of Study: Research |
Subject:
Special
Received: 2025/02/5 | Accepted: 2025/02/9 | Published: 2025/02/9
Received: 2025/02/5 | Accepted: 2025/02/9 | Published: 2025/02/9
References
1. Kakihana W, Akai M, Yamasaki N, Takashima T, Nakazawa K. Changes of joint moments in the gait of normal subjects wearing laterally wedged insoles. American journal of physical medicine & rehabilitation. 2004;83(4):273-8. [DOI:10.1097/01.PHM.0000118035.71195.DE] [PMID]
2. Lidtke R, Muehleman C, Case J, Block J. Relationship between plantar foot pressure and medial knee osteoarthritis. Osteoarthritis Cartilage. 2002;10(7):573-9. [DOI:10.1053/joca.2002.0797] [PMID]
3. Levangie PK, Norkin CC. Joint structure and function: a comprehensive analysis: FA Davis; 2011.
4. Tanaka C, Farah EA. Anatomia funcional das cadeias musculares. Fisioterapia e Pesquisa. 1997;4(1):39-40.
5. Rokninejad M, Hashemi SH. Evaluation of Floor Pressure Distribution in Female Athletes With Tibial Internal Pressure Syndrome. Journal of Sport Biomechanics. 2020;6(3):180-9.
6. Williams III DS, McClay IS, Hamill J, Buchanan TS. Lower extremity kinematic and kinetic differences in runners with high and low arches. Journal of applied biomechanics. 2001;17(2):153-63. [DOI:10.1123/jab.17.2.153]
7. Bennell KL, Bowles K-A, Wang Y, Cicuttini F, Davies-Tuck M, Hinman RS. Higher dynamic medial knee load predicts greater cartilage loss over 12 months in medial knee osteoarthritis. Annals of the rheumatic diseases. 2011;70(10):1770-4. [DOI:10.1136/ard.2010.147082] [PMID]
8. Fregly BJ. Gait modification to treat knee osteoarthritis. HSS journal. 2012;8(1):45-8. [DOI:10.1007/s11420-011-9229-9] [PMID]
9. Hurwitz DE, Sumner DR, Block JA. Bone density, dynamic joint loading and joint degeneration. Cells Tissues Organs. 2001;169(3):201-9. [DOI:10.1159/000047883] [PMID]
10. Landorf KB, Keenan A-M. Efficacy of foot orthoses. What does the literature tell us? Journal of the American Podiatric Medical Association. 2000;90(3):149-58. [DOI:10.7547/87507315-90-3-149] [PMID]
11. Faul F, Erdfelder E, Lang A-G, Buchner A. G* Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior research methods. 2007;39(2):175-91. [DOI:10.3758/BF03193146] [PMID]
12. Zammit GV, Menz HB, Munteanu SE. Reliability of the TekScan MatScan® system for the measurement of plantar forces and pressures during barefoot level walking in healthy adults. Journal of foot and ankle research. 2010;3:1-9. [DOI:10.1186/1757-1146-3-11] [PMID]
13. Thijs Y, De Clercq D, Roosen P, Witvrouw E. Gait-related intrinsic risk factors for patellofemoral pain in novice recreational runners. British journal of sports medicine. 2008;42(6):466-71. [DOI:10.1136/bjsm.2008.046649] [PMID]
14. Khan SS, Khan SJ, Usman J. Effects of toe-out and toe-in gait with varying walking speeds on knee joint mechanics and lower limb energetics. Gait & Posture. 2017;53:185-92. [DOI:10.1016/j.gaitpost.2017.01.022] [PMID]
15. Arndt A, Ekenman I, Westblad P, Lundberg A. Effects of fatigue and load variation on metatarsal deformation measured in vivo during barefoot walking. Journal of biomechanics. 2002;35(5):621-8. [DOI:10.1016/S0021-9290(01)00241-X] [PMID]
16. Williams III DS, Davis IM, Scholz JP, Hamill J, Buchanan TS. High-arched runners exhibit increased leg stiffness compared to low-arched runners. Gait & posture. 2004;19(3):263-9. [DOI:10.1016/S0966-6362(03)00087-0] [PMID]
17. Chuter VH, de Jonge XAJ. Proximal and distal contributions to lower extremity injury: a review of the literature. Gait & posture. 2012;36(1):7-15. [DOI:10.1016/j.gaitpost.2012.02.001] [PMID]
18. Beynnon BD, Murphy DF, Alosa DM. Predictive factors for lateral ankle sprains: a literature review. Journal of athletic training. 2002;37(4):376.
19. Willems T, Witvrouw E, Delbaere K, De Cock A, De Clercq D. Relationship between gait biomechanics and inversion sprains: a prospective study of risk factors. Gait & posture. 2005;21(4):379-87. [DOI:10.1016/j.gaitpost.2004.04.002] [PMID]
20. Wu W-L, Chang J-J, Wu J-H, Guo L-Y, Lin H-T. EMG and plantar pressure patterns after prolonged running. Biomedical Engineering: Applications, Basis and Communications. 2007;19(06):383-8. [DOI:10.4015/S1016237207000483]
21. Nyland J, Kuzemchek S, Parks M, Caborn D. Femoral anteversion influences vastus medialis and gluteus medius EMG amplitude: composite hip abductor EMG amplitude ratios during isometric combined hip abduction-external rotation. Journal of electromyography and kinesiology. 2004;14(2):255-61. [DOI:10.1016/S1050-6411(03)00078-6] [PMID]
22. D'Souza N, Ohashi T, Grayson J, Hiller C, Hutchison L, Simic M. TOE-IN AND TOE-OUT GAIT RETRAINING FOR PEOPLE WITH MEDIAL KNEE OSTEOARTHRITIS: A PILOT RANDOMISED CLINICAL TRIAL. Osteoarthritis and Cartilage. 2022;30:S143-S4. [DOI:10.1016/j.joca.2022.02.181]
23. Hillstrom HJ, Song J, Kraszewski AP, Hafer JF, Mootanah R, Dufour AB, et al. Foot type biomechanics part 1: structure and function of the asymptomatic foot. Gait & posture. 2013;37(3):445-51. [DOI:10.1016/j.gaitpost.2012.09.007] [PMID]
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Journal of Sport Biomechanics
Department of Sport Biomechanics, Faculty of Humanities, Islamic Azad University, Hamedan Branch, Prof. Mousivand Blvd, Imam Khomeini Blvd, Hamedan, Iran.
Journal Tel: +98 81 34494042
Website: http://biomechanics.iauh.ac.ir
Email: sportbiomechanics@iauh.ac.ir
