

Volume 11, Issue 2 (9-2025)
J Sport Biomech 2025, 11(2): 192-206 |
Back to browse issues page



![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Bulbuli A, Chajju N, Ghatage N, Hadgal N. Effect of Blood Flow Restriction Training on Groin Pain in Football Players. J Sport Biomech 2025; 11 (2) :192-206
URL: http://biomechanics.iauh.ac.ir/article-1-394-en.html
URL: http://biomechanics.iauh.ac.ir/article-1-394-en.html



1- KLE Institute of Physiotherapy, Belagavi, Karnataka, India.
Keywords: Adductor strain, Blood flow restriction, Groin pain, Football players, Modified Holmich’s protocol
Full-Text [PDF 1918 kb]
(430 Downloads)
| Abstract (HTML) (1882 Views)
Full-Text: (642 Views)
1. Introduction
Football players experience a higher incidence of lower limb injuries than athletes in many other sports (1). Groin injuries alone account for approximately 10–20% of new injuries sustained by adult male football players, including those at elite and sub-elite levels, making them one of the most prevalent physical complaints in this population (2). In sports medicine, persistent groin pain is a common and often challenging condition to manage. Recovery can be prolonged, delaying an athlete’s full return to sport. Adductor-related pain has been reported to account for 69% of groin injuries in football players and 58% across all sports (3). Consequently, many professional football teams assess players’ hip adductor muscle strength, based on the belief that strength deficits may precede the onset of groin injuries (4). Although some athletes may demonstrate greater resilience due to psychological, physiological, or genetic factors, intrinsic risk factors still contribute significantly to injury occurrence. As such, certain individuals may remain injury-free even when exposed to high-risk conditions (5).
Studies have shown that athletes with lower levels of physical fitness are more susceptible to injury (6). Resistance training is an essential component of any team-sport athlete’s training program, as it enhances muscular strength and endurance, improves power and speed, and reduces the risk of injury (7). Blood Flow Restriction (BFR) training has been shown to elicit muscle hypertrophy responses comparable to those achieved through high-load resistance training (8). Low-load BFR (LL-BFR) exercise, performed at 20–30% of one-repetition maximum (1RM), can produce strength and hypertrophy gains similar to those observed with higher-load protocols (70–85% 1RM). This method reduces mechanical stress on bones and joints, making it a viable option for individuals with musculoskeletal limitations. LL-BFR can therefore help prevent overuse injuries while still effectively promoting muscular adaptation (9).
Groin pain is a frequent complaint among football players, often requiring a comprehensive approach to treatment. Conventional management has included modalities such as transcutaneous electrical nerve stimulation (TENS), therapeutic ultrasound, interferential therapy (IFT), stretching, isometric and strengthening exercises, and sport-specific rehabilitation including skating drills. While Blood Flow Restriction Training (BFRT) has been applied in sports like ice hockey, bodybuilding, and weightlifting, as well as in clinical populations with osteoarthritis, knee pain, and post-anterior cruciate ligament (ACL) reconstruction, its use in football players with groin pain remains underexplored (10–14). Unlike prior studies that have broadly evaluated the efficacy of BFRT in musculoskeletal rehabilitation or general groin pain management, the present study specifically targets football players with groin pain—a group for whom current evidence is limited. Although BFRT has demonstrated promising outcomes in groin-related conditions, there is a clear lack of focused research assessing its direct application in this high-risk athletic population. Therefore, this study aims to address a critical gap in the sports medicine literature by exploring the potential benefits of BFRT for managing groin pain specifically in football players, a group subjected to intense physical demands and a high incidence of injury. The objective of this study was to evaluate the effect of Blood Flow Restriction Training on groin pain in male football players aged 18–30 years, using the Hip and Groin Outcome Scale (HAGOS) and the Visual Analogue Scale (VAS).
2. Methods
2.1 Subjects
The present study employed an experimental pre–post interventional design with a final sample size of 16 participants. The required sample size was calculated using the following formula:
n = [(Zα + Zβ)² × 2 × σ²] / d²
Where:
• Zα = 1.96 (corresponding to a 5% significance level)
• Zβ = 0.84 (corresponding to 80% statistical power)
• σ = 6 (estimated standard deviation)
• d = 6 (expected minimum difference)
Substituting the values into the formula:
n = [(1.96 + 0.84)² × 2 × 6²] / 6²
n = [2.8² × 2 × 36] / 36
n = [7.84 × 72] / 36
n = 564.48 / 36 = 15.68 ≈ 16
To account for a potential 10% dropout rate, 18 participants were initially recruited through probability-based random sampling to ensure the desired sample of 16 subjects. Ethical approval was obtained from the institutional ethics review committee prior to the commencement of the study. Participants were male football players aged 18 to 30 years from Belagavi city, all experiencing groin pain. Screening was conducted using the Visual Analogue Scale (VAS), and only those with scores of 3 or higher were included. Individuals with a history of hypertension, diabetes mellitus, peripheral vascular disease, neurological disorders, skin conditions, or cancer were excluded from participation. Eligible players were further evaluated using the Copenhagen Hip and Groin Outcome Score (HAGOS), which quantitatively assessed groin pain and functional status. The intervention involved a structured Blood Flow Restriction (BFR) training protocol tailored for this athletic population.
2.2 Procedure
All subjects were screened according to the inclusion and exclusion criteria. Written informed consent was obtained in the participants’ native language. Basic demographic data were collected prior to the intervention. BFR cuffs used in the study were 3 inches wide and 71 inches long. The cuff pressure was set at 60–70% of arterial occlusion pressure (AOP) and was progressively increased during sessions, ranging from 160 to 200 mmHg (13).
2.3 Intervention
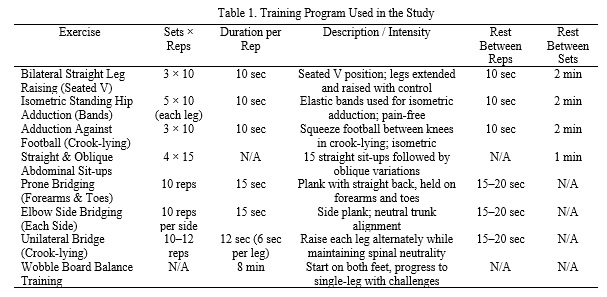
The intervention followed a modified Holmich protocol (Table 1) and was administered by certified physiotherapists. A treatment diary was maintained to monitor adherence. The intervention was delivered over 4 weeks, totaling 12 sessions. A BFR tourniquet was applied over the groin area to restrict venous outflow while maintaining arterial inflow. During each session, the therapist demonstrated the prescribed exercises. Cuff pressure was gradually increased throughout the session, and occlusion was maintained during the exercise sets and released during rest intervals (13).
2.4 Outcome Measures
Copenhagen Hip and Groin Outcome Score (HAGOS) is a 37-item questionnaire designed to assess hip and groin-related pain, symptoms, physical function in daily life and sport, participation in physical activities, and quality of life. It has demonstrated excellent test–retest reliability with an intraclass correlation coefficient (ICC) ranging from 0.82 to 0.91. Participants completed the questionnaire both pre- and post-intervention (15).
Visual Analogue Scale (VAS) is a 0–10 scale used to assess pain intensity. Participants were instructed to mark the number that best represented their current level of pain, where higher scores indicate greater pain severity and lower scores suggest less pain (16).
2.5 Statistical Analysis
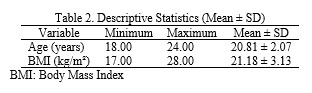
Statistical analysis was performed using SPSS version 23. The Shapiro–Wilk test confirmed the normal distribution of the data. Descriptive statistics were used to summarize the participants’ baseline characteristics, including age and body mass index (BMI). A paired sample t-test was conducted to compare the pre- and post-intervention scores for both outcome measures.
3. Results
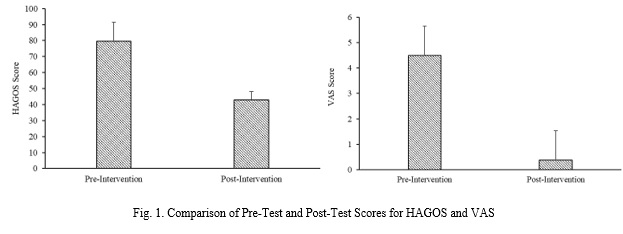
The baseline characteristics of the participants, including age and body mass index (BMI), are presented in Table 2. A paired sample t-test was conducted to compare pre-test and post-test scores for both outcome measures. The analysis revealed a statistically significant difference between pre-intervention and post-intervention HAGOS scores (p < 0.001), with a substantial reduction in mean scores and decreased variability after the intervention (Table 3). The calculated effect size (Cohen’s d) was 3.65, which is considered a very large effect based on standard benchmarks (Table 3). Similarly, the comparison of pre-test and post-test VAS scores showed a marked reduction in pain following the intervention, with the mean score dropping from 4.50 to 0.38 and a corresponding effect size of 4.66, indicating a very large effect (Table 4). The post-intervention scores also demonstrated greater consistency, as indicated by the lower standard deviation compared to the pre-test values (Table 4). These improvements are clearly illustrated in Fig. 1, which displays the reductions in both HAGOS and VAS scores following the four-week intervention period. Overall, the findings confirm that the application of blood flow restriction training produced statistically and clinically significant improvements in groin pain and function among the participants.


4. Discussion
This study evaluated the effectiveness of blood flow restriction (BFR) training combined with the Modified Holmich protocol in reducing groin pain among football players. A total of 16 participants underwent 12 sessions over a 4-week period, with pre- and post-intervention assessments using the HAGOS and VAS outcome measures. The results demonstrated significant reductions in groin pain and improvements in functional outcomes, confirming the therapeutic value of BFR training in musculoskeletal rehabilitation. Our findings align with and expand upon existing literature demonstrating the benefits of BFR. While prior studies have predominantly focused on the performance-enhancing effects of BFR—particularly in adolescents and younger athletes—our study highlights its clinical relevance in injury management (12). The observed reductions in HAGOS and VAS scores underscore BFR’s dual utility: not only can it enhance strength and hypertrophy, but it also serves as an effective rehabilitation modality. These findings reinforce the need to consider age-specific and goal-oriented adaptations when applying BFR training across athletic populations.
In contrast to studies that focused on aerobic capacity improvements through BFR (17), our investigation emphasized pain reduction and functional recovery in athletes with groin-related discomfort. This distinction illustrates the versatility of BFR, demonstrating its potential for both performance enhancement and therapeutic use. The convergence of positive outcomes across these studies supports the integration of BFR into comprehensive athletic conditioning and rehabilitation programs. Further comparison with strength training studies in older adults shows how exercise interventions, though applied to different populations, can yield beneficial outcomes. While such studies emphasize improvements in quality of life and functional mobility in seniors, our research targets injury-specific rehabilitation in young athletes (18). This contrast highlights the adaptability of exercise-based therapy and the importance of tailoring interventions to the physiological characteristics and needs of the target group. A randomized controlled trial investigating resistance training with and without BFR in older adults reported superior gains in knee extensor strength and functional performance in the BFR group, as measured by timed up and go (TUG) and sit-to-stand (STS) tests (19). Although the participant populations and study designs differ, the evidence from both studies supports BFR’s efficacy—whether for enhancing strength in the elderly or managing groin pain in athletes. These complementary findings reinforce BFR’s broad applicability across clinical and performance domains.
Additionally, BFR has been widely explored in the context of post-surgical rehabilitation, particularly following anterior cruciate ligament (ACL) reconstruction. Studies have shown its effectiveness in preserving muscle mass and accelerating recovery (20). In our study, football players with groin pain experienced difficulty in training and competition, but the integration of BFR training with targeted exercises led to rapid improvements in pain and function within a relatively short timeframe. This suggests that BFR may offer a time-efficient and effective intervention for a variety of musculoskeletal conditions beyond surgical contexts. Moreover, prior studies using the modified Holmich protocol alone have shown effectiveness in managing adductor-related groin pain. However, our findings suggest that combining BFR training with the modified Holmich regimen results in superior outcomes—specifically, faster pain reduction, greater functional gains, and earlier return to sport (21). This integrated approach appears to enhance both the speed and extent of recovery, underscoring its potential as a highly effective treatment strategy for groin-related injuries in athletic populations.
This study has several limitations that should be acknowledged. First, the exclusion of female participants limits the generalizability of the findings to the broader athletic population. Second, the absence of follow-up evaluations restricts our understanding of the long-term effects of the intervention. Additionally, the lack of a control group and the omission of functional performance testing further constrain the interpretation of the results and the ability to assess practical improvements in athletic function. Future studies should aim to include a more diverse sample, incorporating both male and female participants, to enhance external validity. The inclusion of a randomized control group and follow-up assessments would help determine the sustainability of the intervention’s effects over time. Furthermore, integrating functional performance tests would allow for a more comprehensive evaluation of recovery and return-to-play readiness. To improve long-term muscle healing, future research could also explore the addition of a progressive strengthening phase to the Modified Holmich protocol.
5. Conclusion
Based on the statistical findings, it can be concluded that blood flow restriction (BFR) training has a significant effect on reducing groin pain in football players. When combined with the Modified Holmich protocol, BFR training effectively promotes muscle repair and enhances functional recovery. This intervention demonstrates strong potential as a time-efficient and clinically valuable approach for accelerating rehabilitation in athletes with groin-related injuries.
Acknowledgments
I would like to thank KLE University's Institute of Physiotherapy, Belagavi, for allowing me to conduct this study.
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be addressed in this research.
Funding
This research did not receive any grants from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed equally to preparing the article.
Conflicts of interest
The authors declared no conflict of interest.
Football players experience a higher incidence of lower limb injuries than athletes in many other sports (1). Groin injuries alone account for approximately 10–20% of new injuries sustained by adult male football players, including those at elite and sub-elite levels, making them one of the most prevalent physical complaints in this population (2). In sports medicine, persistent groin pain is a common and often challenging condition to manage. Recovery can be prolonged, delaying an athlete’s full return to sport. Adductor-related pain has been reported to account for 69% of groin injuries in football players and 58% across all sports (3). Consequently, many professional football teams assess players’ hip adductor muscle strength, based on the belief that strength deficits may precede the onset of groin injuries (4). Although some athletes may demonstrate greater resilience due to psychological, physiological, or genetic factors, intrinsic risk factors still contribute significantly to injury occurrence. As such, certain individuals may remain injury-free even when exposed to high-risk conditions (5).
Studies have shown that athletes with lower levels of physical fitness are more susceptible to injury (6). Resistance training is an essential component of any team-sport athlete’s training program, as it enhances muscular strength and endurance, improves power and speed, and reduces the risk of injury (7). Blood Flow Restriction (BFR) training has been shown to elicit muscle hypertrophy responses comparable to those achieved through high-load resistance training (8). Low-load BFR (LL-BFR) exercise, performed at 20–30% of one-repetition maximum (1RM), can produce strength and hypertrophy gains similar to those observed with higher-load protocols (70–85% 1RM). This method reduces mechanical stress on bones and joints, making it a viable option for individuals with musculoskeletal limitations. LL-BFR can therefore help prevent overuse injuries while still effectively promoting muscular adaptation (9).
Groin pain is a frequent complaint among football players, often requiring a comprehensive approach to treatment. Conventional management has included modalities such as transcutaneous electrical nerve stimulation (TENS), therapeutic ultrasound, interferential therapy (IFT), stretching, isometric and strengthening exercises, and sport-specific rehabilitation including skating drills. While Blood Flow Restriction Training (BFRT) has been applied in sports like ice hockey, bodybuilding, and weightlifting, as well as in clinical populations with osteoarthritis, knee pain, and post-anterior cruciate ligament (ACL) reconstruction, its use in football players with groin pain remains underexplored (10–14). Unlike prior studies that have broadly evaluated the efficacy of BFRT in musculoskeletal rehabilitation or general groin pain management, the present study specifically targets football players with groin pain—a group for whom current evidence is limited. Although BFRT has demonstrated promising outcomes in groin-related conditions, there is a clear lack of focused research assessing its direct application in this high-risk athletic population. Therefore, this study aims to address a critical gap in the sports medicine literature by exploring the potential benefits of BFRT for managing groin pain specifically in football players, a group subjected to intense physical demands and a high incidence of injury. The objective of this study was to evaluate the effect of Blood Flow Restriction Training on groin pain in male football players aged 18–30 years, using the Hip and Groin Outcome Scale (HAGOS) and the Visual Analogue Scale (VAS).
2. Methods
2.1 Subjects
The present study employed an experimental pre–post interventional design with a final sample size of 16 participants. The required sample size was calculated using the following formula:
n = [(Zα + Zβ)² × 2 × σ²] / d²
Where:
• Zα = 1.96 (corresponding to a 5% significance level)
• Zβ = 0.84 (corresponding to 80% statistical power)
• σ = 6 (estimated standard deviation)
• d = 6 (expected minimum difference)
Substituting the values into the formula:
n = [(1.96 + 0.84)² × 2 × 6²] / 6²
n = [2.8² × 2 × 36] / 36
n = [7.84 × 72] / 36
n = 564.48 / 36 = 15.68 ≈ 16
To account for a potential 10% dropout rate, 18 participants were initially recruited through probability-based random sampling to ensure the desired sample of 16 subjects. Ethical approval was obtained from the institutional ethics review committee prior to the commencement of the study. Participants were male football players aged 18 to 30 years from Belagavi city, all experiencing groin pain. Screening was conducted using the Visual Analogue Scale (VAS), and only those with scores of 3 or higher were included. Individuals with a history of hypertension, diabetes mellitus, peripheral vascular disease, neurological disorders, skin conditions, or cancer were excluded from participation. Eligible players were further evaluated using the Copenhagen Hip and Groin Outcome Score (HAGOS), which quantitatively assessed groin pain and functional status. The intervention involved a structured Blood Flow Restriction (BFR) training protocol tailored for this athletic population.
2.2 Procedure
All subjects were screened according to the inclusion and exclusion criteria. Written informed consent was obtained in the participants’ native language. Basic demographic data were collected prior to the intervention. BFR cuffs used in the study were 3 inches wide and 71 inches long. The cuff pressure was set at 60–70% of arterial occlusion pressure (AOP) and was progressively increased during sessions, ranging from 160 to 200 mmHg (13).
2.3 Intervention
The intervention followed a modified Holmich protocol (Table 1) and was administered by certified physiotherapists. A treatment diary was maintained to monitor adherence. The intervention was delivered over 4 weeks, totaling 12 sessions. A BFR tourniquet was applied over the groin area to restrict venous outflow while maintaining arterial inflow. During each session, the therapist demonstrated the prescribed exercises. Cuff pressure was gradually increased throughout the session, and occlusion was maintained during the exercise sets and released during rest intervals (13).
2.4 Outcome Measures
Copenhagen Hip and Groin Outcome Score (HAGOS) is a 37-item questionnaire designed to assess hip and groin-related pain, symptoms, physical function in daily life and sport, participation in physical activities, and quality of life. It has demonstrated excellent test–retest reliability with an intraclass correlation coefficient (ICC) ranging from 0.82 to 0.91. Participants completed the questionnaire both pre- and post-intervention (15).
Visual Analogue Scale (VAS) is a 0–10 scale used to assess pain intensity. Participants were instructed to mark the number that best represented their current level of pain, where higher scores indicate greater pain severity and lower scores suggest less pain (16).
2.5 Statistical Analysis
Statistical analysis was performed using SPSS version 23. The Shapiro–Wilk test confirmed the normal distribution of the data. Descriptive statistics were used to summarize the participants’ baseline characteristics, including age and body mass index (BMI). A paired sample t-test was conducted to compare the pre- and post-intervention scores for both outcome measures.
3. Results
The baseline characteristics of the participants, including age and body mass index (BMI), are presented in Table 2. A paired sample t-test was conducted to compare pre-test and post-test scores for both outcome measures. The analysis revealed a statistically significant difference between pre-intervention and post-intervention HAGOS scores (p < 0.001), with a substantial reduction in mean scores and decreased variability after the intervention (Table 3). The calculated effect size (Cohen’s d) was 3.65, which is considered a very large effect based on standard benchmarks (Table 3). Similarly, the comparison of pre-test and post-test VAS scores showed a marked reduction in pain following the intervention, with the mean score dropping from 4.50 to 0.38 and a corresponding effect size of 4.66, indicating a very large effect (Table 4). The post-intervention scores also demonstrated greater consistency, as indicated by the lower standard deviation compared to the pre-test values (Table 4). These improvements are clearly illustrated in Fig. 1, which displays the reductions in both HAGOS and VAS scores following the four-week intervention period. Overall, the findings confirm that the application of blood flow restriction training produced statistically and clinically significant improvements in groin pain and function among the participants.
4. Discussion
This study evaluated the effectiveness of blood flow restriction (BFR) training combined with the Modified Holmich protocol in reducing groin pain among football players. A total of 16 participants underwent 12 sessions over a 4-week period, with pre- and post-intervention assessments using the HAGOS and VAS outcome measures. The results demonstrated significant reductions in groin pain and improvements in functional outcomes, confirming the therapeutic value of BFR training in musculoskeletal rehabilitation. Our findings align with and expand upon existing literature demonstrating the benefits of BFR. While prior studies have predominantly focused on the performance-enhancing effects of BFR—particularly in adolescents and younger athletes—our study highlights its clinical relevance in injury management (12). The observed reductions in HAGOS and VAS scores underscore BFR’s dual utility: not only can it enhance strength and hypertrophy, but it also serves as an effective rehabilitation modality. These findings reinforce the need to consider age-specific and goal-oriented adaptations when applying BFR training across athletic populations.
In contrast to studies that focused on aerobic capacity improvements through BFR (17), our investigation emphasized pain reduction and functional recovery in athletes with groin-related discomfort. This distinction illustrates the versatility of BFR, demonstrating its potential for both performance enhancement and therapeutic use. The convergence of positive outcomes across these studies supports the integration of BFR into comprehensive athletic conditioning and rehabilitation programs. Further comparison with strength training studies in older adults shows how exercise interventions, though applied to different populations, can yield beneficial outcomes. While such studies emphasize improvements in quality of life and functional mobility in seniors, our research targets injury-specific rehabilitation in young athletes (18). This contrast highlights the adaptability of exercise-based therapy and the importance of tailoring interventions to the physiological characteristics and needs of the target group. A randomized controlled trial investigating resistance training with and without BFR in older adults reported superior gains in knee extensor strength and functional performance in the BFR group, as measured by timed up and go (TUG) and sit-to-stand (STS) tests (19). Although the participant populations and study designs differ, the evidence from both studies supports BFR’s efficacy—whether for enhancing strength in the elderly or managing groin pain in athletes. These complementary findings reinforce BFR’s broad applicability across clinical and performance domains.
Additionally, BFR has been widely explored in the context of post-surgical rehabilitation, particularly following anterior cruciate ligament (ACL) reconstruction. Studies have shown its effectiveness in preserving muscle mass and accelerating recovery (20). In our study, football players with groin pain experienced difficulty in training and competition, but the integration of BFR training with targeted exercises led to rapid improvements in pain and function within a relatively short timeframe. This suggests that BFR may offer a time-efficient and effective intervention for a variety of musculoskeletal conditions beyond surgical contexts. Moreover, prior studies using the modified Holmich protocol alone have shown effectiveness in managing adductor-related groin pain. However, our findings suggest that combining BFR training with the modified Holmich regimen results in superior outcomes—specifically, faster pain reduction, greater functional gains, and earlier return to sport (21). This integrated approach appears to enhance both the speed and extent of recovery, underscoring its potential as a highly effective treatment strategy for groin-related injuries in athletic populations.
This study has several limitations that should be acknowledged. First, the exclusion of female participants limits the generalizability of the findings to the broader athletic population. Second, the absence of follow-up evaluations restricts our understanding of the long-term effects of the intervention. Additionally, the lack of a control group and the omission of functional performance testing further constrain the interpretation of the results and the ability to assess practical improvements in athletic function. Future studies should aim to include a more diverse sample, incorporating both male and female participants, to enhance external validity. The inclusion of a randomized control group and follow-up assessments would help determine the sustainability of the intervention’s effects over time. Furthermore, integrating functional performance tests would allow for a more comprehensive evaluation of recovery and return-to-play readiness. To improve long-term muscle healing, future research could also explore the addition of a progressive strengthening phase to the Modified Holmich protocol.
5. Conclusion
Based on the statistical findings, it can be concluded that blood flow restriction (BFR) training has a significant effect on reducing groin pain in football players. When combined with the Modified Holmich protocol, BFR training effectively promotes muscle repair and enhances functional recovery. This intervention demonstrates strong potential as a time-efficient and clinically valuable approach for accelerating rehabilitation in athletes with groin-related injuries.
Acknowledgments
I would like to thank KLE University's Institute of Physiotherapy, Belagavi, for allowing me to conduct this study.
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be addressed in this research.
Funding
This research did not receive any grants from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed equally to preparing the article.
Conflicts of interest
The authors declared no conflict of interest.
Type of Study: Research |
Subject:
General
Received: 2025/06/9 | Accepted: 2025/06/17 | Published: 2025/06/25
Received: 2025/06/9 | Accepted: 2025/06/17 | Published: 2025/06/25
References
1. Mohamadi A, Letafatkar A, Hosseini SH, Heshmati S. The effect of six weeks of hamstring eccentric exercises on the postural control and knee joint proprioception in adolescent football players. Journal of Sport Biomechanics. 2017;3(3):15-25.
2. Thorborg K, Rathleff MS, Petersen P, Branci S, Hölmich P. Prevalence and severity of hip and groin pain in sub-elite male football: a cross-sectional cohort study of 695 players. Scandinavian Journal of Medicine & Science in Sports. 2017;27(1):107-114. [DOI:10.1111/sms.12623] [PMID]
3. Waldén M, Hägglund M, Ekstrand J. The epidemiology of groin injury in senior football: a systematic review of prospective studies. British Journal of Sports Medicine. 2015;49(12):792-797. [DOI:10.1136/bjsports-2015-094705] [PMID]
4. Crow JF, Pearce AJ, Veale JP, VanderWesthuizen D, Coburn PT, Pizzari T. Hip adductor muscle strength is reduced preceding and during the onset of groin pain in elite junior Australian football players. Journal of Science and Medicine in Sport. 2010;13(2):202-204. [DOI:10.1016/j.jsams.2009.03.007] [PMID]
5. Wilkerson GB, Giles JL, Seibel DK. Prediction of core and lower extremity strains and sprains in collegiate football players: a preliminary study. Journal of Athletic Training. 2012;47(3):264-272. [DOI:10.4085/1062-6050-47.3.17] [PMID]
6. Eslami A, Sahebozamani M, Bahiraei S. The effect of the FIFA 11+ Kids warm-up training program on lower limb injury prevention and football player performance: a systematic review. Journal of Sport Biomechanics. 2023;9(1):2-15. [DOI:10.61186/JSportBiomech.9.1.2]
7. The effects of supplementary low-load blood flow restriction training on morphological and performance-based adaptations in team sport athletes. Journal of Strength and Conditioning Research. 2017;31(8):2147-2154. [DOI:10.1519/JSC.0000000000001671] [PMID]
8. Hughes L, Paton B, Rosenblatt B, Gissane C, Patterson SD. Blood flow restriction training in clinical musculoskeletal rehabilitation: a systematic review and meta-analysis. British Journal of Sports Medicine. 2017;51(13):1003-1011. [DOI:10.1136/bjsports-2016-097071] [PMID]
9. Centner C, Wiegel P, Gollhofer A, König D. Effects of blood flow restriction training on muscular strength and hypertrophy in older individuals: a systematic review and meta-analysis. Sports Medicine. 2019;49(1):95-108. [DOI:10.1007/s40279-018-1013-2] [PMID]
10. Scott BR, Loenneke JP, Slattery KM, Dascombe BJ. Blood flow restricted exercise for athletes: a review of available evidence. Journal of Science and Medicine in Sport. 2016;19(5):360-367. [DOI:10.1016/j.jsams.2015.04.014] [PMID]
11. Weir A, Jansen JA, van de Port IG, Van de Sande HB, Tol JL, Backx FJ. Manual or exercise therapy for long-standing adductor-related groin pain: a randomised controlled clinical trial. Manual Therapy. 2011;16(2):148-154. [DOI:10.1016/j.math.2010.09.001] [PMID]
12. Luebbers PE, Witte EV, Oshel JQ, Butler MS. Effects of practical blood flow restriction training on adolescent lower-body strength. Journal of Strength and Conditioning Research. 2019;33(10):2674-2683. [DOI:10.1519/JSC.0000000000002302] [PMID]
13. Barber-Westin S, Noyes FR. Blood flow-restricted training for lower extremity muscle weakness due to knee pathology: a systematic review. Sports Health. 2019;11(1):69-83. [DOI:10.1177/1941738118811337] [PMID]
14. Erickson LN, Lucas KCH, Davis KA, et al. Effect of blood flow restriction training on quadriceps muscle strength, morphology, physiology, and knee biomechanics before and after anterior cruciate ligament reconstruction: protocol for a randomized clinical trial. Physical Therapy. 2019;99(8):1010-1019. [DOI:10.1093/ptj/pzz062] [PMID]
15. Thorborg K, Hölmich P, Christensen R, Petersen J, Roos EM. The Copenhagen Hip and Groin Outcome Score (HAGOS): development and validation according to the COSMIN checklist [published correction appears in British Journal of Sports Medicine. 2011 Jul;45(9):742]. British Journal of Sports Medicine. 2011;45(6):478-491. [DOI:10.1136/bjsm.2010.080937] [PMID]
16. Johnson EW. Visual analog scale (VAS). American Journal of Physical Medicine & Rehabilitation. 2001;80(10):717. [DOI:10.1097/00002060-200110000-00001] [PMID]
17. Amani AR, Sadeghi H, Afsharnezhad T. Interval training with blood flow restriction on aerobic performance among young soccer players at transition phase. Montenegrin Journal of Sports Science and Medicine. 2018;7(2). [DOI:10.26773/mjssm.180901]
18. Kovač T, Marček T, Šarkanj B, et al. Fullerol C60 (OH)24 nanoparticles and drought impact on wheat (Triticum aestivum L.) during growth and infection with Aspergillus flavus. Journal of Fungi (Basel). 2021;7(3):236. [DOI:10.3390/jof7030236] [PMID]
19. Libardi CA, Chacon-Mikahil MP, Cavaglieri CR, et al. Effect of concurrent training with blood flow restriction in the elderly. International Journal of Sports Medicine. 2015;36(5):395-399. [DOI:10.1055/s-0034-1390496] [PMID]
20. Charles D, White R, Reyes C, Palmer D. A systematic review of the effects of blood flow restriction training on quadriceps muscle atrophy and circumference post ACL reconstruction. International Journal of Sports Physical Therapy. 2020;15(6):882-891. [DOI:10.26603/ijspt20200882] [PMID]
21. Yousefzadeh A, Shadmehr A, Olyaei GR, Naseri N, Khazaeipour Z. The effect of therapeutic exercise on long-standing adductor-related groin pain in athletes: modified Hölmich protocol. Rehabilitation Research and Practice. 2018; 2018:8146819. [DOI:10.1155/2018/8146819] [PMID]
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Journal of Sport Biomechanics
Department of Sport Biomechanics, Faculty of Humanities, Islamic Azad University, Hamedan Branch, Prof. Mousivand Blvd, Imam Khomeini Blvd, Hamedan, Iran.
Journal Tel: +98 81 34494042
Website: http://biomechanics.iauh.ac.ir
Email: sportbiomechanics@iauh.ac.ir
