

Volume 12, Issue 2 (9-2026)
J Sport Biomech 2026, 12(2): 302-319 |
Back to browse issues page


![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Asghari V, Farahpour N, Robbins S, Moisan G, Majlesi M. Kinematic Changes of Lower-Limb Joints During Walking in Individuals with Chronic Ankle Instability on Flat and Inclined Surfaces. J Sport Biomech 2026; 12 (2) :302-319
URL: http://biomechanics.iauh.ac.ir/article-1-436-en.html
URL: http://biomechanics.iauh.ac.ir/article-1-436-en.html



1- Department of Sport Biomechanics, Faculty of Sport Sciences, Bu-Ali Sina University, Hamedan, Iran.
2- Department of Physiotherapy, McGill University, Montreal, QC, Canada.
3- Department of Human Kinetics, Université du Québec à Trois-Rivières, Trois-Rivières, Canada.
4- Department of Sport Biomechanics, Ha.C. Islamic Azad University, Hamedan, Iran.
2- Department of Physiotherapy, McGill University, Montreal, QC, Canada.
3- Department of Human Kinetics, Université du Québec à Trois-Rivières, Trois-Rivières, Canada.
4- Department of Sport Biomechanics, Ha.C. Islamic Azad University, Hamedan, Iran.
Keywords: Chronic ankle instability, Joint kinematics, Angular velocity, Spatiotemporal parameters, Range of motion
Full-Text [PDF 2119 kb]
(318 Downloads)
| Abstract (HTML) (1064 Views)
Full-Text: (758 Views)
Extended Abstract
1. Introduction
Lateral ankle sprain is one of the most common musculoskeletal injuries, accounting for more than 80% of all ankle injuries (1). Approximately 40% of affected individuals subsequently develop chronic ankle instability (CAI), a condition characterized by persistent symptoms and long-term functional limitations (1,2). Individuals with CAI commonly experience recurrent sprains, sensations of giving way, pain, swelling, weakness, restricted joint motion, and limitations in physical activity (3–5). Pathoanatomically, injury primarily involves the lateral ligament complex of the ankle, particularly the anterior talofibular (ATFL) and calcaneofibular (CFL) ligaments (6,7). Damage to these ligaments also disrupts mechanoreceptors, leading to impaired proprioception and deficits in joint position sense and movement control (4).
Gait analysis provides valuable insight into these impairments, as walking tasks can reveal CAI-related neuromuscular and biomechanical deficiencies (7). Persistent abnormal gait patterns may contribute to the chronicity of the condition by altering joint loading and movement strategies (3). Consequently, individuals with CAI often exhibit altered gait patterns, reduced dynamic stability, and an increased susceptibility to recurrent ankle sprains (4,11). Previous studies have reported kinematic differences in ankle motion during gait in individuals with CAI (6,11). Commonly reported alterations include shorter step length, prolonged stance phase, restricted range of motion, increased ankle inversion, and greater internal rotation compared with healthy individuals (4,11). These changes are associated with impaired neuromuscular control and reduced motor performance (12). To compensate for ankle instability, individuals with CAI appear to adopt movement strategies that rely more heavily on proximal joints, particularly the knee and hip (12,13). During walking, reduced knee flexion, decreased knee external rotation, and increased hip flexion and abduction have been reported in individuals with CAI compared with healthy controls (15–19). While gait assessment on stable surfaces provides important biomechanical insights (15), rehabilitation programs increasingly emphasize unstable or challenging walking conditions, as these environments place greater demands on proprioception and motor control (20). Despite extensive research on lower-extremity biomechanics in CAI (17,23,24), findings regarding joint kinematics remain inconsistent (8,12,25,26). These inconsistencies may be attributed to methodological limitations, including small sample sizes, exclusive focus on level walking, and failure to examine multi-joint kinematic behavior simultaneously.
Therefore, the purpose of the present study was to analyze lower-limb kinematic gait patterns in individuals with CAI during walking on both level and inclined surfaces and to compare these patterns with those of healthy controls. It was hypothesized that: (1) ankle and foot movement patterns would differ significantly between individuals with CAI and healthy controls, and (2) knee and hip kinematics would also be significantly altered, reflecting compensatory adaptations.
2. Methods
This semi-experimental study included 37 physically active male participants aged 20–40 years, comprising 18 individuals with chronic ankle instability (CAI group) and 19 healthy controls. Participants with CAI were recruited from orthopedic clinics and sports centers, whereas control participants were recruited from eligible volunteers. The diagnosis of CAI was confirmed by an orthopedic specialist in accordance with the International Ankle Consortium criteria and included a history of recurrent ankle sprains, a Cumberland Ankle Instability Tool (CAIT) score below 24 (27), and functional limitations identified using the Foot and Ankle Ability Measure (FAAM). Exclusion criteria for both groups included a history of lower-limb surgery or the presence of other musculoskeletal or neurological disorders. Three-dimensional gait analysis was performed using an eight-camera Qualisys motion capture system sampling at 200 Hz. A total of 62 reflective markers were placed on anatomical landmarks of the lower extremities based on a modified Rizzoli marker set. Ground reaction forces were recorded using two Kistler force plates synchronized with the motion capture system. Participants were instructed to walk under two conditions: on a level surface and on a 15° inclined surface (28–30). Four successful trials were recorded for each condition.
Kinematic data were processed using Qualisys Track Manager and Visual3D software. Marker trajectories were filtered and time-normalized to 101 data points representing 0–100% of the gait cycle. Statistical parametric mapping (SPM) was used to compare continuous kinematic waveforms between groups across the gait cycle. Additionally, multivariate analysis of variance (MANOVA) was applied for discrete variable comparisons. Statistical significance was set at p ≤ 0.05.
3. Results
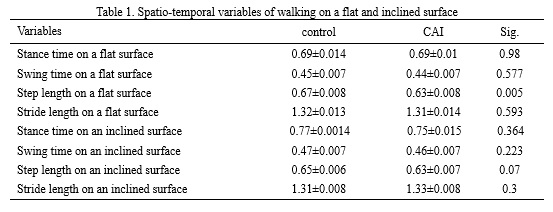
Analysis revealed key differences between the CAI and control groups during walking. The CAI group The analysis revealed several key differences between the CAI and control groups during walking. On the level surface, individuals with CAI demonstrated a significantly shorter step length compared with controls (mean difference: 0.034 m, p = 0.005) (Table 1). On the inclined surface, this difference was marginal and did not reach statistical significance (p = 0.07). No significant between-group differences were observed in joint range of motion (ROM) for any lower-limb joint under either walking condition.
Kinematic waveform analysis identified substantial joint-specific alterations. During level walking, the CAI group exhibited reduced hip extension, increased hip flexion, and reduced hip abduction compared with controls. These differences became more pronounced during inclined walking, with the CAI group demonstrating greater hip flexion, reduced hip adduction, decreased knee external rotation, and increased ankle inversion across multiple phases of the gait cycle. In addition, altered ankle angular velocities were observed during inclined walking in the CAI group. Although overall ROM remained unchanged, individuals with CAI displayed compensatory movement strategies that were amplified under the increased mechanical demands of inclined walking.
1. Introduction
Lateral ankle sprain is one of the most common musculoskeletal injuries, accounting for more than 80% of all ankle injuries (1). Approximately 40% of affected individuals subsequently develop chronic ankle instability (CAI), a condition characterized by persistent symptoms and long-term functional limitations (1,2). Individuals with CAI commonly experience recurrent sprains, sensations of giving way, pain, swelling, weakness, restricted joint motion, and limitations in physical activity (3–5). Pathoanatomically, injury primarily involves the lateral ligament complex of the ankle, particularly the anterior talofibular (ATFL) and calcaneofibular (CFL) ligaments (6,7). Damage to these ligaments also disrupts mechanoreceptors, leading to impaired proprioception and deficits in joint position sense and movement control (4).
Gait analysis provides valuable insight into these impairments, as walking tasks can reveal CAI-related neuromuscular and biomechanical deficiencies (7). Persistent abnormal gait patterns may contribute to the chronicity of the condition by altering joint loading and movement strategies (3). Consequently, individuals with CAI often exhibit altered gait patterns, reduced dynamic stability, and an increased susceptibility to recurrent ankle sprains (4,11). Previous studies have reported kinematic differences in ankle motion during gait in individuals with CAI (6,11). Commonly reported alterations include shorter step length, prolonged stance phase, restricted range of motion, increased ankle inversion, and greater internal rotation compared with healthy individuals (4,11). These changes are associated with impaired neuromuscular control and reduced motor performance (12). To compensate for ankle instability, individuals with CAI appear to adopt movement strategies that rely more heavily on proximal joints, particularly the knee and hip (12,13). During walking, reduced knee flexion, decreased knee external rotation, and increased hip flexion and abduction have been reported in individuals with CAI compared with healthy controls (15–19). While gait assessment on stable surfaces provides important biomechanical insights (15), rehabilitation programs increasingly emphasize unstable or challenging walking conditions, as these environments place greater demands on proprioception and motor control (20). Despite extensive research on lower-extremity biomechanics in CAI (17,23,24), findings regarding joint kinematics remain inconsistent (8,12,25,26). These inconsistencies may be attributed to methodological limitations, including small sample sizes, exclusive focus on level walking, and failure to examine multi-joint kinematic behavior simultaneously.
Therefore, the purpose of the present study was to analyze lower-limb kinematic gait patterns in individuals with CAI during walking on both level and inclined surfaces and to compare these patterns with those of healthy controls. It was hypothesized that: (1) ankle and foot movement patterns would differ significantly between individuals with CAI and healthy controls, and (2) knee and hip kinematics would also be significantly altered, reflecting compensatory adaptations.
2. Methods
This semi-experimental study included 37 physically active male participants aged 20–40 years, comprising 18 individuals with chronic ankle instability (CAI group) and 19 healthy controls. Participants with CAI were recruited from orthopedic clinics and sports centers, whereas control participants were recruited from eligible volunteers. The diagnosis of CAI was confirmed by an orthopedic specialist in accordance with the International Ankle Consortium criteria and included a history of recurrent ankle sprains, a Cumberland Ankle Instability Tool (CAIT) score below 24 (27), and functional limitations identified using the Foot and Ankle Ability Measure (FAAM). Exclusion criteria for both groups included a history of lower-limb surgery or the presence of other musculoskeletal or neurological disorders. Three-dimensional gait analysis was performed using an eight-camera Qualisys motion capture system sampling at 200 Hz. A total of 62 reflective markers were placed on anatomical landmarks of the lower extremities based on a modified Rizzoli marker set. Ground reaction forces were recorded using two Kistler force plates synchronized with the motion capture system. Participants were instructed to walk under two conditions: on a level surface and on a 15° inclined surface (28–30). Four successful trials were recorded for each condition.
Kinematic data were processed using Qualisys Track Manager and Visual3D software. Marker trajectories were filtered and time-normalized to 101 data points representing 0–100% of the gait cycle. Statistical parametric mapping (SPM) was used to compare continuous kinematic waveforms between groups across the gait cycle. Additionally, multivariate analysis of variance (MANOVA) was applied for discrete variable comparisons. Statistical significance was set at p ≤ 0.05.
3. Results
Analysis revealed key differences between the CAI and control groups during walking. The CAI group The analysis revealed several key differences between the CAI and control groups during walking. On the level surface, individuals with CAI demonstrated a significantly shorter step length compared with controls (mean difference: 0.034 m, p = 0.005) (Table 1). On the inclined surface, this difference was marginal and did not reach statistical significance (p = 0.07). No significant between-group differences were observed in joint range of motion (ROM) for any lower-limb joint under either walking condition.
Kinematic waveform analysis identified substantial joint-specific alterations. During level walking, the CAI group exhibited reduced hip extension, increased hip flexion, and reduced hip abduction compared with controls. These differences became more pronounced during inclined walking, with the CAI group demonstrating greater hip flexion, reduced hip adduction, decreased knee external rotation, and increased ankle inversion across multiple phases of the gait cycle. In addition, altered ankle angular velocities were observed during inclined walking in the CAI group. Although overall ROM remained unchanged, individuals with CAI displayed compensatory movement strategies that were amplified under the increased mechanical demands of inclined walking.
4. Discussion
This study examined lower-limb gait kinematics in individuals with chronic ankle instability during walking on level and inclined surfaces. The hypothesis that individuals with CAI would exhibit altered movement patterns compared with healthy controls was partially supported. The most consistent finding was a significant reduction in step length during level walking, which is consistent with previous findings reported by Delahunt et al. (2006) (41). This adaptation may reflect a strategy to enhance stability by reducing joint loading and lowering the center of mass, thereby minimizing the risk of episodes of giving way. However, this finding contrasts with studies reporting no differences in step length (20,32,33), underscoring the variability of compensatory strategies among individuals with CAI. An unexpected but notable finding was the absence of significant differences in total joint ROM at the hip, knee, and ankle between groups on either surface. This result aligns with the findings of Hertel and Corbett (2019) (35) but contrasts with studies reporting reduced ankle ROM and strength deficits in individuals with CAI (4,6). Such discrepancies may be attributable to methodological differences, particularly the use of dynamic gait analysis in the present study versus static or isolated joint assessments in previous research (4). The most pronounced kinematic alterations were observed at the hip joint. Across both walking conditions, individuals with CAI demonstrated increased hip flexion and reduced hip abduction/adduction, supporting previous observations by Son et al. (2019) (17).
These findings strongly suggest a compensatory strategy characterized by increased reliance on proximal joints to maintain stability and control movement, likely driven by sensorimotor deficits and reduced confidence in ankle stability. Overall, individuals with CAI exhibit altered movement patterns that extend beyond the ankle joint, with compensatory adaptations affecting the hip and knee, particularly during more demanding tasks such as inclined walking. These findings highlight the need for comprehensive rehabilitation strategies that address the entire kinetic chain rather than focusing solely on the ankle. Effective rehabilitation programs should incorporate proprioceptive training, strengthening of proximal and calf musculature, and gait retraining aimed at correcting compensatory movement patterns and improving dynamic stability in real-world walking environments.
Ethical Considerations
Compliance with ethical guidelines
This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki. All participants (or their parents/legal guardians, where applicable) provided written informed consent after receiving a full explanation of the study procedures and objectives. The study protocol was approved by the institutional research ethics committee.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Authors' contributions
All authors contributed to the study conception and design, data collection, data analysis, and drafting or critical revision of the manuscript. All authors read and approved the final version of the manuscript and take responsibility for its content.
Conflicts of interest
The authors declare that they have no conflicts of interest, financial or otherwise, related to this study.
This study examined lower-limb gait kinematics in individuals with chronic ankle instability during walking on level and inclined surfaces. The hypothesis that individuals with CAI would exhibit altered movement patterns compared with healthy controls was partially supported. The most consistent finding was a significant reduction in step length during level walking, which is consistent with previous findings reported by Delahunt et al. (2006) (41). This adaptation may reflect a strategy to enhance stability by reducing joint loading and lowering the center of mass, thereby minimizing the risk of episodes of giving way. However, this finding contrasts with studies reporting no differences in step length (20,32,33), underscoring the variability of compensatory strategies among individuals with CAI. An unexpected but notable finding was the absence of significant differences in total joint ROM at the hip, knee, and ankle between groups on either surface. This result aligns with the findings of Hertel and Corbett (2019) (35) but contrasts with studies reporting reduced ankle ROM and strength deficits in individuals with CAI (4,6). Such discrepancies may be attributable to methodological differences, particularly the use of dynamic gait analysis in the present study versus static or isolated joint assessments in previous research (4). The most pronounced kinematic alterations were observed at the hip joint. Across both walking conditions, individuals with CAI demonstrated increased hip flexion and reduced hip abduction/adduction, supporting previous observations by Son et al. (2019) (17).
These findings strongly suggest a compensatory strategy characterized by increased reliance on proximal joints to maintain stability and control movement, likely driven by sensorimotor deficits and reduced confidence in ankle stability. Overall, individuals with CAI exhibit altered movement patterns that extend beyond the ankle joint, with compensatory adaptations affecting the hip and knee, particularly during more demanding tasks such as inclined walking. These findings highlight the need for comprehensive rehabilitation strategies that address the entire kinetic chain rather than focusing solely on the ankle. Effective rehabilitation programs should incorporate proprioceptive training, strengthening of proximal and calf musculature, and gait retraining aimed at correcting compensatory movement patterns and improving dynamic stability in real-world walking environments.
Ethical Considerations
Compliance with ethical guidelines
This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki. All participants (or their parents/legal guardians, where applicable) provided written informed consent after receiving a full explanation of the study procedures and objectives. The study protocol was approved by the institutional research ethics committee.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Authors' contributions
All authors contributed to the study conception and design, data collection, data analysis, and drafting or critical revision of the manuscript. All authors read and approved the final version of the manuscript and take responsibility for its content.
Conflicts of interest
The authors declare that they have no conflicts of interest, financial or otherwise, related to this study.
Type of Study: Research |
Subject:
Special
Received: 2025/09/13 | Accepted: 2026/01/20 | Published: 2026/01/31
Received: 2025/09/13 | Accepted: 2026/01/20 | Published: 2026/01/31
References
1. Jeon HG, Lee I, Kim H, Jeong H, Ha S, Kim BH, et al. Impact of fatiguing exercises on movement strategies in chronic ankle instability, lateral ankle sprain copers, and controls. Journal of Sports Science and Medicine. 2025;24(1):116. [DOI:10.52082/jssm.2025.116]
2. Elabd OM, Elabd AM, El-Azez MSA, Taha MM, Mohammed AH. Impact of chronic ankle instability on gait loading strategy in individuals with chronic ankle instability: a comparative study. Journal of NeuroEngineering and Rehabilitation. 2024;21(1):185. [DOI:10.1186/s12984-024-01478-8]
3. Kim BH, Kang TK, Lee SY. Integrating biofeedback in dynamic biomechanical gait training for chronic ankle instability. Applied Sciences. 2025;15(4):1688. [DOI:10.3390/app15041688]
4. Jagadale S, Shinde S, Aphale S. Analyzing lower limb muscle imbalance patterns associated with chronic ankle instability. Cureus. 2025;17(1). [DOI:10.7759/cureus.77529]
5. Abdalqadir Mohammed H, Abdullah Ali R, Ali Mohammed A, Ali Faiaq Habib K. The immediate effect of kinesiotaping on lower limb movement patterns in soccer athletes with chronic ankle instability: a quasi-experimental study. Journal of Sport Biomechanics. 2026;11(4):378-90. [DOI:10.61882/JSportBiomech.11.4.378]
6. Wang S, Ruan Y, Wang K, Chang F, Chen B, Zhang N, et al. New insights into chronic ankle instability: an in vivo evaluation of three-dimensional motion and stability of the ankle joint complex. Frontiers in Bioengineering and Biotechnology. 2025;13:1556291. [DOI:10.3389/fbioe.2025.1556291]
7. Yu P, Cen X, Mei Q, Wang A, Gu Y, Fernandez J. Differences in intra-foot movement strategies during locomotive tasks among chronic ankle instability, copers and healthy individuals. Journal of Biomechanics. 2024;162:111865. [DOI:10.1016/j.jbiomech.2023.111865]
8. Herb C, Custer L, Blemker S, Saliba S, Hart J, Hertel J. Gait kinematics and kinetics in patients with chronic ankle instability and healthy controls: a statistical parametric mapping analysis. The Foot. 2024;59:102089. [DOI:10.1016/j.foot.2024.102089]
9. Mohammadi Yaghoubi U, Farahpour N, Mansoorizadeh M, Moisan G. Evaluation of single-leg balance during landing from 20- and 40-centimeter heights in individuals with and without chronic ankle instability. Journal of Sport Biomechanics. 2025;11(1):2-19. [DOI:10.61186/JSportBiomech.11.1.2]
10. Mohammadpour N, Rezaie I, Hadadi M. The relationship between core muscles dysfunction and chronic ankle instability: a review. Journal of Sport Biomechanics. 2019;5(2):72-81. [DOI:10.32598/biomechanics.5.2.4]
11. Luan L, Orth D, Newman P, Adams R, El-Ansary D, Han J. Do individuals with ankle instability show altered lower extremity kinematics and kinetics during walking? A systematic review and meta-analysis. Physiotherapy. 2024;125:101420. [DOI:10.1016/j.physio.2024.101420]
12. Brown C. Foot clearance in walking and running in individuals with ankle instability. The American Journal of Sports Medicine. 2011;39(8):1769-77. [DOI:10.1177/0363546511408872]
13. Theisen A, Day J. Chronic ankle instability leads to lower extremity kinematic changes during landing tasks: a systematic review. International Journal of Exercise Science. 2019;12(1):24. [DOI:10.70252/DTNP3988]
14. Riemann BL. Is there a link between chronic ankle instability and postural instability? Journal of Athletic Training. 2002;37(4):386.
15. Altun A, Dixon S, Rice H. Task-specific differences in lower limb biomechanics during dynamic movements in individuals with chronic ankle instability compared with controls. Gait & Posture. 2024;113:265-71. [DOI:10.1016/j.gaitpost.2024.07.004]
16. Moisan G, Mainville C, Descarreaux M, Cantin V. Kinematic, kinetic and electromyographic differences between young adults with and without chronic ankle instability during walking. Journal of Electromyography and Kinesiology. 2020;51:102399. [DOI:10.1016/j.jelekin.2020.102399]
17. Son SJ, Kim H, Seeley MK, Hopkins JT. Altered walking neuromechanics in patients with chronic ankle instability. Journal of Athletic Training. 2019;54(6):684-97. [DOI:10.4085/1062-6050-478-17]
18. Koshino Y, Ishida T, Yamanaka M, Ezawa Y, Okunuki T, Kobayashi T, et al. Kinematics and muscle activities of the lower limb during a side-cutting task in subjects with chronic ankle instability. Knee Surgery, Sports Traumatology, Arthroscopy. 2016;24(4):1071-80. [DOI:10.1007/s00167-015-3745-y]
19. Moisan G, Descarreaux M, Cantin V. Effects of chronic ankle instability on kinetics, kinematics and muscle activity during walking and running: a systematic review. Gait & Posture. 2017;52:381-99. [DOI:10.1016/j.gaitpost.2016.11.037]
20. Lee GW, Lee J, Shin SW, Kim J. Quantification of gait characteristics and muscle activation in patients with chronic ankle instability during walking on sand: a randomized crossover trial. Medicine. 2024;103(50):e40902. [DOI:10.1097/MD.0000000000040902]
21. Négyesi J, Kovács B, Petró B, Salman DN, Khandoker A, Katona P, et al. Side dominance and eye patches obscuring half of the visual field do not affect walking kinematics. Scientific Reports. 2025;15(1):6189. [DOI:10.1038/s41598-025-90936-x]
22. Van den Hoorn W. Evaluation of the dynamical structures of postural control: new insights into motor adaptation in ageing and pain. 2018.
23. Moisan G, Mainville C, Descarreaux M, Cantin V. Lower limb biomechanics in individuals with chronic ankle instability during gait: a case-control study. Journal of Foot and Ankle Research. 2021;14(1):36. [DOI:10.1186/s13047-021-00476-6]
24. Chinn L, Dicharry J, Hertel J. Ankle kinematics of individuals with chronic ankle instability while walking and jogging on a treadmill in shoes. Physical Therapy in Sport. 2013;14(4):232-9. [DOI:10.1016/j.ptsp.2012.10.001]
25. Ruan Y, Wang S, Zhang N, Jiang Z, Mei N, Li P, et al. In vivo analysis of ankle joint kinematics and ligament deformation of chronic ankle instability patients during level walking. Frontiers in Bioengineering and Biotechnology. 2024;12:1441005. [DOI:10.3389/fbioe.2024.1441005]
26. Koshino Y, Yamanaka M, Ezawa Y, Ishida T, Kobayashi T, Samukawa M, et al. Lower limb joint motion during a cross cutting movement differs in individuals with and without chronic ankle instability. Physical Therapy in Sport. 2014;15(4):242-8. [DOI:10.1016/j.ptsp.2013.12.001]
27. Gribble PA, Bleakley CM, Caulfield BM, Docherty CL, Fourchet F, Fong DT-P, et al. Evidence review for the 2016 International Ankle Consortium consensus statement on the prevalence, impact and long-term consequences of lateral ankle sprains. British Journal of Sports Medicine. 2016;50(24):1496-505.
https://doi.org/10.1136/bjsports-2016-096188 [DOI:10.1136/bjsports-2016-096189]
28. Strutzenberger G, Leutgeb L, Claußen L, Schwameder H. Gait on slopes: differences in temporo-spatial, kinematic and kinetic gait parameters between walking on a ramp and on a treadmill. Gait & Posture. 2022;91:73-8. [DOI:10.1016/j.gaitpost.2021.09.196]
29. Strutzenberger G, Claußen L, Schwameder H. Analysis of sloped gait: how many steps are needed to reach steady-state walking speed after gait initiation? Gait & Posture. 2021;83:167-73. [DOI:10.1016/j.gaitpost.2020.09.030]
30. Nieuwenhuijzen P, Grüneberg C, Duysens J. Mechanically induced ankle inversion during human walking and jumping. Journal of Neuroscience Methods. 2002;117(2):133-40. [DOI:10.1016/S0165-0270(02)00089-4]
31. Dubbeldam R, Buurke J, Simons C, Groothuis-Oudshoorn C, Baan H, Nene A, et al. The effects of walking speed on forefoot, hindfoot and ankle joint motion. Clinical Biomechanics. 2010;25(8):796-801. [DOI:10.1016/j.clinbiomech.2010.06.007]
32. Moreno-Hernández A, Rodríguez-Reyes G, Quiñones-Urióstegui I, Núñez-Carrera L, Pérez-SanPablo AI. Temporal and spatial gait parameters analysis in non-pathological Mexican children. Gait & Posture. 2010;32(1):78-81. [DOI:10.1016/j.gaitpost.2010.03.010]
33. Lythgo N, Wilson C, Galea M. Basic gait and symmetry measures for primary school-aged children and young adults whilst walking barefoot and with shoes. Gait & Posture. 2009;30(4):502-6. [DOI:10.1016/j.gaitpost.2009.07.119]
34. Xu X, Bowtell J, Fong DT, Young WR, Williams GK. Kinematics of balance controls in people with chronic ankle instability during unilateral stance on a moving platform. Scientific Reports. 2025;15(1):1126. [DOI:10.1038/s41598-025-85220-x]
35. Hertel J, Corbett RO. An updated model of chronic ankle instability. Journal of Athletic Training. 2019;54(6):572-88. [DOI:10.4085/1062-6050-344-18]
36. Koldenhoven RM, Hart J, Saliba S, Abel MF, Hertel J. Gait kinematics and kinetics at three walking speeds in individuals with chronic ankle instability and ankle sprain copers. Gait & Posture. 2019;74:169-75. [DOI:10.1016/j.gaitpost.2019.09.010]
37. Monaghan K, Delahunt E, Caulfield B. Ankle function during gait in patients with chronic ankle instability compared to controls. Clinical Biomechanics. 2006;21(2):168-74. [DOI:10.1016/j.clinbiomech.2005.09.004]
38. Drewes LK, McKeon PO, Paolini G, Riley P, Kerrigan DC, Ingersoll CD, et al. Altered ankle kinematics and shank-rear-foot coupling in those with chronic ankle instability. Journal of Sport Rehabilitation. 2009;18(3):375-88. [DOI:10.1123/jsr.18.3.375]
39. Koldenhoven RM, Jaffri AH, DeJong AF, Abel M, Hart J, Saliba S, et al. Gait biofeedback and impairment-based rehabilitation for chronic ankle instability. Scandinavian Journal of Medicine & Science in Sports. 2021;31(1):193-204. [DOI:10.1111/sms.13823]
40. Lee I, Ha S, Chae S, Jeong HS, Lee SY. Altered biomechanics in individuals with chronic ankle instability compared with copers and controls during gait. Journal of Athletic Training. 2022;57(8):760-70. [DOI:10.4085/1062-6050-0605.20]
41. Northeast L, Gautrey CN, Bottoms L, Hughes G, Mitchell AC, Greenhalgh A. Full gait cycle analysis of lower limb and trunk kinematics and muscle activations during walking in participants with and without ankle instability. Gait & Posture. 2018;64:114-8. [DOI:10.1016/j.gaitpost.2018.06.001]
42. Delahunt E, Monaghan K, Caulfield B. Altered neuromuscular control and ankle joint kinematics during walking in subjects with functional instability of the ankle joint. The American Journal of Sports Medicine. 2006;34(12):1970-6. [DOI:10.1177/0363546506290989]
43. Kakihana W, Torii S, Akai M, Nakazawa K, Fukano M, Naito K. Effect of a lateral wedge on joint moments during gait in subjects with recurrent ankle sprain. American Journal of Physical Medicine & Rehabilitation. 2005;84(11):858-64. [DOI:10.1097/01.phm.0000179519.65254.37]
44. Fraser JJ, Hart JM, Saliba SF, Park JS, Tumperi M, Hertel J. Multisegmented ankle-foot kinematics during gait initiation in ankle sprains and chronic ankle instability. Clinical Biomechanics. 2019;68:80-8. [DOI:10.1016/j.clinbiomech.2019.05.017]
45. Yen S-C, Corkery MB, Donohoe A, Grogan M, Wu Y-N. Feedback and feedforward control during walking in individuals with chronic ankle instability. Journal of Orthopaedic & Sports Physical Therapy. 2016;46(9):775-83. [DOI:10.2519/jospt.2016.6403]
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Journal of Sport Biomechanics
Department of Sport Biomechanics, Faculty of Humanities, Islamic Azad University, Hamedan Branch, Prof. Mousivand Blvd, Imam Khomeini Blvd, Hamedan, Iran.
Journal Tel: +98 81 34494042
Website: http://biomechanics.iauh.ac.ir
Email: sportbiomechanics@iauh.ac.ir
