

Volume 12, Issue 1 (6-2026)
J Sport Biomech 2026, 12(1): 70-88 |
Back to browse issues page


![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Ahanjan S, Dashti Rostami K, Jalalvand A. Investigation of Chronic Ankle Instability in Athletes Using Artificial Neural Networks. J Sport Biomech 2026; 12 (1) :70-88
URL: http://biomechanics.iauh.ac.ir/article-1-444-en.html
URL: http://biomechanics.iauh.ac.ir/article-1-444-en.html



1- Department of Sport Sciences and Health, Amirkabir University of Technology, Tehran, Iran.
2- Department of Motor Behavior and Biomechanics, Faculty of Sport Sciences, University of Mazandaran, Babolsar, Iran.
3- Department of Sport Biomechanics, Ha.C., Islamic Azad University, Hamedan, Iran.
2- Department of Motor Behavior and Biomechanics, Faculty of Sport Sciences, University of Mazandaran, Babolsar, Iran.
3- Department of Sport Biomechanics, Ha.C., Islamic Azad University, Hamedan, Iran.
Full-Text [PDF 1846 kb]
(270 Downloads)
| Abstract (HTML) (1061 Views)
Full-Text: (340 Views)
Extended Abstract
1. Introduction
In the past decade, scientific progress has been profoundly driven by advances in computational hardware and algorithmic development. High-speed information processing has accelerated data-driven discoveries across a wide range of disciplines. Despite these technological breakthroughs, the human brain remains the most efficient and adaptable model for information processing. Consequently, much of artificial intelligence research has focused on developing computational systems that emulate brain-inspired mechanisms for problem-solving (1, 2). An artificial neural network (ANN) is an information-processing architecture modeled after the biological nervous system. These networks consist of interconnected processing units capable of learning complex nonlinear relationships from data, enabling them to perform classification, prediction, and pattern recognition tasks (2).
Chronic ankle instability (CAI) is a common and debilitating consequence of acute lateral ankle sprains, often associated with recurrent “giving-way” episodes, restricted range of motion, reduced performance, and pain (3). Epidemiological evidence indicates that a considerable proportion of individuals experience persistent instability and functional limitations following an initial sprain (4, 5). Clinically, CAI is traditionally categorized into two domains: mechanical instability, resulting from ligamentous laxity, and functional instability, arising from deficits in proprioception and neuromuscular control. However, recent perspectives emphasize that CAI represents a multifactorial condition encompassing anatomical, biomechanical, and sensorimotor impairments (5, 6). Emerging studies have demonstrated that machine learning and neural network models can effectively predict athletic performance based on physiological and biomechanical parameters. These models often outperform traditional statistical approaches in talent identification, injury prediction, and performance profiling across various sports disciplines (7). Moreover, recent literature highlights the combined influence of joint geometry (mortise and syndesmosis), ligament integrity, talar positioning, and sensorimotor feedback on ankle stability. Consequently, modern rehabilitation strategies advocate a comprehensive approach that simultaneously addresses ligamentous laxity, joint mechanics, and neuromuscular deficits (5, 8). Dynamic balance deficits, delayed peroneal muscle activation, and mechanical indices—such as increased inversion laxity or anterior talar translation—have been identified as major predictors of CAI. Multivariate approaches integrating these parameters demonstrate superior classification accuracy compared with single functional tests (4, 9). Recently, neural network and machine learning algorithms have been increasingly applied to predict sports injuries and monitor performance. Accumulating evidence suggests that these tools can identify athletes at elevated risk by modeling the complex, nonlinear interactions among multiple risk factors (7, 10). However, limited research has explored the use of artificial neural networks specifically for predicting chronic ankle instability in athletes, underscoring the need for further investigation.
2. Methods
This study included forty male athletes from various sports disciplines, all of whom had at least two years of national league experience. Twenty athletes with chronic ankle instability (CAI) were selected based on a history of severe lateral ankle sprains, recurrent episodes of instability, and absence of prior rehabilitation. The control group consisted of twenty athletes with no previous history of ankle injury. Exclusion criteria for the CAI group included bilateral instability, ankle fractures, and prior ankle surgery. Participants’ anthropometric characteristics were first measured following standardized procedures. Height was recorded in a barefoot, upright standing position with the heels, hips, and shoulders touching a vertical surface (11). Body weight was measured using a calibrated digital scale while participants stood barefoot and in light clothing; weight was recorded to the nearest 0.1 kg (12). Forefoot width was determined using a footprint method on graph paper. While standing barefoot and bearing full weight, the widest medial and lateral points of the forefoot were marked, and the distance between them was measured in millimeters (13). Foot pronation was evaluated using the navicular drop test, which quantifies the difference in navicular bone height between non–weight-bearing (seated) and weight-bearing (standing) positions (14).
Active and passive ranges of motion (ROM) for dorsiflexion and plantarflexion were assessed using a standard goniometer while participants sat with their legs hanging freely.
The medial malleolus served as the axis, and the goniometer arms were aligned accordingly. Participants performed the movement for active ROM, while the examiner performed it for passive ROM (15, 16). Similarly, active and passive inversion ROM was measured with the goniometer axis placed at the medial head of the first metatarsal and the arms positioned at 90°. Active measurements were performed by the participant, and passive measurements by the examiner (15, 16). Eversion ROM was assessed in the same position, with the goniometer axis located at the lateral head of the fifth metatarsal; the stationary arm aligned with the lower leg, and the moving arm placed along the plantar surface of the foot. Each measurement was repeated twice, and if the difference between trials exceeded five degrees, a third measurement was taken; the mean of the two closest values was recorded (17). Static postural control was evaluated using a modified Romberg test, in which participants stood on one leg with the opposite knee flexed to 90°, arms crossed over the chest, and eyes closed. Balance was considered normal if the participant maintained the position for more than 15 seconds, and abnormal otherwise. This test has demonstrated high intra-rater reliability (R = 0.89) (18, 19). Agility performance was assessed using the Illinois Agility Test, which involves a 10-meter-long and 5-meter-wide course marked with cones (20). Each participant completed the course twice at maximal speed while maintaining accuracy, coordination, and balance, and the average time of both trials was recorded. Statistical analyses were conducted using independent t-tests to compare groups and discriminant analysis to identify variables with the greatest discriminative power.
3. Results
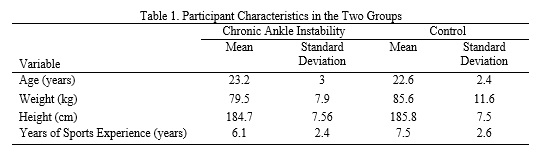
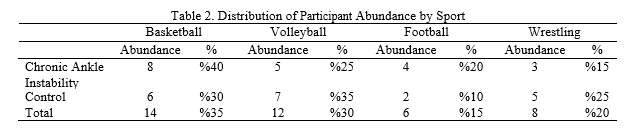
Table 1 summarizes the descriptive characteristics of the participants, including age, body mass, height, and years of sports experience, across the two study groups. Table 2 presents the distribution of athletes according to their respective sports disciplines. A total of forty data sets were analyzed, each comprising fourteen input variables and one output variable. Several neural-network configurations were tested to identify the model that produced the highest predictive accuracy. The optimal structure consisted of a feed-forward back-propagation network with fourteen input neurons, twelve hidden neurons, and one output neuron. Sigmoid activation functions were employed in both the hidden and output layers to enable nonlinear mapping and to constrain the output values between 0 and 1. The network was trained using 70% of the available data, while the remaining 30% were reserved for testing. The convergence of the training process was confirmed by the progressive reduction in error and the close correspondence between predicted and actual outputs. The training-error plot and output-comparison curve demonstrated high model stability and precision. The linear regression analysis yielded an R value of 0.9997, indicating an excellent fit between the predicted and experimental data and confirming the superior predictive performance of the neural-network model.
1. Introduction
In the past decade, scientific progress has been profoundly driven by advances in computational hardware and algorithmic development. High-speed information processing has accelerated data-driven discoveries across a wide range of disciplines. Despite these technological breakthroughs, the human brain remains the most efficient and adaptable model for information processing. Consequently, much of artificial intelligence research has focused on developing computational systems that emulate brain-inspired mechanisms for problem-solving (1, 2). An artificial neural network (ANN) is an information-processing architecture modeled after the biological nervous system. These networks consist of interconnected processing units capable of learning complex nonlinear relationships from data, enabling them to perform classification, prediction, and pattern recognition tasks (2).
Chronic ankle instability (CAI) is a common and debilitating consequence of acute lateral ankle sprains, often associated with recurrent “giving-way” episodes, restricted range of motion, reduced performance, and pain (3). Epidemiological evidence indicates that a considerable proportion of individuals experience persistent instability and functional limitations following an initial sprain (4, 5). Clinically, CAI is traditionally categorized into two domains: mechanical instability, resulting from ligamentous laxity, and functional instability, arising from deficits in proprioception and neuromuscular control. However, recent perspectives emphasize that CAI represents a multifactorial condition encompassing anatomical, biomechanical, and sensorimotor impairments (5, 6). Emerging studies have demonstrated that machine learning and neural network models can effectively predict athletic performance based on physiological and biomechanical parameters. These models often outperform traditional statistical approaches in talent identification, injury prediction, and performance profiling across various sports disciplines (7). Moreover, recent literature highlights the combined influence of joint geometry (mortise and syndesmosis), ligament integrity, talar positioning, and sensorimotor feedback on ankle stability. Consequently, modern rehabilitation strategies advocate a comprehensive approach that simultaneously addresses ligamentous laxity, joint mechanics, and neuromuscular deficits (5, 8). Dynamic balance deficits, delayed peroneal muscle activation, and mechanical indices—such as increased inversion laxity or anterior talar translation—have been identified as major predictors of CAI. Multivariate approaches integrating these parameters demonstrate superior classification accuracy compared with single functional tests (4, 9). Recently, neural network and machine learning algorithms have been increasingly applied to predict sports injuries and monitor performance. Accumulating evidence suggests that these tools can identify athletes at elevated risk by modeling the complex, nonlinear interactions among multiple risk factors (7, 10). However, limited research has explored the use of artificial neural networks specifically for predicting chronic ankle instability in athletes, underscoring the need for further investigation.
2. Methods
This study included forty male athletes from various sports disciplines, all of whom had at least two years of national league experience. Twenty athletes with chronic ankle instability (CAI) were selected based on a history of severe lateral ankle sprains, recurrent episodes of instability, and absence of prior rehabilitation. The control group consisted of twenty athletes with no previous history of ankle injury. Exclusion criteria for the CAI group included bilateral instability, ankle fractures, and prior ankle surgery. Participants’ anthropometric characteristics were first measured following standardized procedures. Height was recorded in a barefoot, upright standing position with the heels, hips, and shoulders touching a vertical surface (11). Body weight was measured using a calibrated digital scale while participants stood barefoot and in light clothing; weight was recorded to the nearest 0.1 kg (12). Forefoot width was determined using a footprint method on graph paper. While standing barefoot and bearing full weight, the widest medial and lateral points of the forefoot were marked, and the distance between them was measured in millimeters (13). Foot pronation was evaluated using the navicular drop test, which quantifies the difference in navicular bone height between non–weight-bearing (seated) and weight-bearing (standing) positions (14).
Active and passive ranges of motion (ROM) for dorsiflexion and plantarflexion were assessed using a standard goniometer while participants sat with their legs hanging freely.
The medial malleolus served as the axis, and the goniometer arms were aligned accordingly. Participants performed the movement for active ROM, while the examiner performed it for passive ROM (15, 16). Similarly, active and passive inversion ROM was measured with the goniometer axis placed at the medial head of the first metatarsal and the arms positioned at 90°. Active measurements were performed by the participant, and passive measurements by the examiner (15, 16). Eversion ROM was assessed in the same position, with the goniometer axis located at the lateral head of the fifth metatarsal; the stationary arm aligned with the lower leg, and the moving arm placed along the plantar surface of the foot. Each measurement was repeated twice, and if the difference between trials exceeded five degrees, a third measurement was taken; the mean of the two closest values was recorded (17). Static postural control was evaluated using a modified Romberg test, in which participants stood on one leg with the opposite knee flexed to 90°, arms crossed over the chest, and eyes closed. Balance was considered normal if the participant maintained the position for more than 15 seconds, and abnormal otherwise. This test has demonstrated high intra-rater reliability (R = 0.89) (18, 19). Agility performance was assessed using the Illinois Agility Test, which involves a 10-meter-long and 5-meter-wide course marked with cones (20). Each participant completed the course twice at maximal speed while maintaining accuracy, coordination, and balance, and the average time of both trials was recorded. Statistical analyses were conducted using independent t-tests to compare groups and discriminant analysis to identify variables with the greatest discriminative power.
3. Results
Table 1 summarizes the descriptive characteristics of the participants, including age, body mass, height, and years of sports experience, across the two study groups. Table 2 presents the distribution of athletes according to their respective sports disciplines. A total of forty data sets were analyzed, each comprising fourteen input variables and one output variable. Several neural-network configurations were tested to identify the model that produced the highest predictive accuracy. The optimal structure consisted of a feed-forward back-propagation network with fourteen input neurons, twelve hidden neurons, and one output neuron. Sigmoid activation functions were employed in both the hidden and output layers to enable nonlinear mapping and to constrain the output values between 0 and 1. The network was trained using 70% of the available data, while the remaining 30% were reserved for testing. The convergence of the training process was confirmed by the progressive reduction in error and the close correspondence between predicted and actual outputs. The training-error plot and output-comparison curve demonstrated high model stability and precision. The linear regression analysis yielded an R value of 0.9997, indicating an excellent fit between the predicted and experimental data and confirming the superior predictive performance of the neural-network model.
4. Discussion
The findings of this study showed no significant difference in body mass index (BMI) between athletes with and without chronic ankle instability (CAI). Previous research on military populations has reported contrasting results. Waterman et al. (2010) found that individuals who sustained ankle sprains exhibited higher mean height, weight, and BMI than healthy controls, suggesting that elevated BMI may increase the risk of ankle sprains in military settings (21). This association has been attributed to a greater moment of inertia around the ankle joint, which imposes higher mechanical stress on surrounding tissues—particularly when external loads such as backpacks are carried (22). The discrepancy between the current findings and those of Milgrom et al. (23) may reflect differences in methodology, participant characteristics, sample size, or measurement techniques. A significant difference was observed in forefoot width between groups: athletes with CAI demonstrated a greater mean forefoot width (10.59 ± 0.48 cm) compared with controls (10.12 ± 0.41 cm). This aligns with prior evidence suggesting that wider feet are associated with an increased risk of recurrent ankle sprains (22, 24). Biomechanically, a wider forefoot may lengthen the inversion lever arm, thereby increasing the mechanical load on the lateral ligaments of the ankle and predisposing the joint to instability.
No significant difference was found in foot pronation between groups, consistent with the findings of Martin et al. (2013) and Maeda et al. (2023) (25, 26). The conventional static classification of foot type (pronated, supinated, or neutral) may not adequately reflect dynamic biomechanical abnormalities under injury-relevant conditions. Hence, future studies should employ more sensitive, task-specific assessments of foot–ground interaction during functional and high-risk movements to better characterize injury susceptibility. Similarly, no significant differences were observed in active or passive dorsiflexion range of motion (ROM) between the groups, corroborating the findings of Vomacka et al. (2019) (27). Active inversion ROM also did not differ significantly, likely due to sufficient neuromuscular control and proprioceptive feedback in both groups. However, a significant difference was identified in passive inversion ROM, which was greater in the CAI group (41.2 ± 2.87°) than in controls (38.8 ± 3.05°). This result is consistent with Hubbard et al. (2007) (28) and may indicate deficient passive restraint provided by non-contractile tissues, such as the lateral ligaments and joint capsule, that were inadequately rehabilitated following the initial injury. No significant group differences were found in Illinois Agility Test performance, echoing the observations of Sarvestan and Svoboda (2019) (29). Although athletes with CAI often report subtle or subjective instability, these symptoms do not necessarily impair their measurable functional agility.
The discriminant analysis model incorporating eight variables effectively differentiated between the CAI and healthy groups. The model achieved a correct classification rate of 85% for healthy participants, 80% for those with CAI, and 82.5% overall. Among the predictors, forefoot width (r = 0.54) and passive inversion ROM (r = 0.51) demonstrated the highest correlations with the discriminant function, underscoring their substantial contribution to chronic ankle instability. Collectively, these findings suggest that increased forefoot width and excessive passive inversion range of motion are key biomechanical risk factors for CAI and should be targeted in preventive and rehabilitative strategies for athletes.
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be addressed in this research.
Funding
This research did not receive any grants from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed equally to preparing the article.
Conflicts of interest
The authors declared no conflict of interest.
The findings of this study showed no significant difference in body mass index (BMI) between athletes with and without chronic ankle instability (CAI). Previous research on military populations has reported contrasting results. Waterman et al. (2010) found that individuals who sustained ankle sprains exhibited higher mean height, weight, and BMI than healthy controls, suggesting that elevated BMI may increase the risk of ankle sprains in military settings (21). This association has been attributed to a greater moment of inertia around the ankle joint, which imposes higher mechanical stress on surrounding tissues—particularly when external loads such as backpacks are carried (22). The discrepancy between the current findings and those of Milgrom et al. (23) may reflect differences in methodology, participant characteristics, sample size, or measurement techniques. A significant difference was observed in forefoot width between groups: athletes with CAI demonstrated a greater mean forefoot width (10.59 ± 0.48 cm) compared with controls (10.12 ± 0.41 cm). This aligns with prior evidence suggesting that wider feet are associated with an increased risk of recurrent ankle sprains (22, 24). Biomechanically, a wider forefoot may lengthen the inversion lever arm, thereby increasing the mechanical load on the lateral ligaments of the ankle and predisposing the joint to instability.
No significant difference was found in foot pronation between groups, consistent with the findings of Martin et al. (2013) and Maeda et al. (2023) (25, 26). The conventional static classification of foot type (pronated, supinated, or neutral) may not adequately reflect dynamic biomechanical abnormalities under injury-relevant conditions. Hence, future studies should employ more sensitive, task-specific assessments of foot–ground interaction during functional and high-risk movements to better characterize injury susceptibility. Similarly, no significant differences were observed in active or passive dorsiflexion range of motion (ROM) between the groups, corroborating the findings of Vomacka et al. (2019) (27). Active inversion ROM also did not differ significantly, likely due to sufficient neuromuscular control and proprioceptive feedback in both groups. However, a significant difference was identified in passive inversion ROM, which was greater in the CAI group (41.2 ± 2.87°) than in controls (38.8 ± 3.05°). This result is consistent with Hubbard et al. (2007) (28) and may indicate deficient passive restraint provided by non-contractile tissues, such as the lateral ligaments and joint capsule, that were inadequately rehabilitated following the initial injury. No significant group differences were found in Illinois Agility Test performance, echoing the observations of Sarvestan and Svoboda (2019) (29). Although athletes with CAI often report subtle or subjective instability, these symptoms do not necessarily impair their measurable functional agility.
The discriminant analysis model incorporating eight variables effectively differentiated between the CAI and healthy groups. The model achieved a correct classification rate of 85% for healthy participants, 80% for those with CAI, and 82.5% overall. Among the predictors, forefoot width (r = 0.54) and passive inversion ROM (r = 0.51) demonstrated the highest correlations with the discriminant function, underscoring their substantial contribution to chronic ankle instability. Collectively, these findings suggest that increased forefoot width and excessive passive inversion range of motion are key biomechanical risk factors for CAI and should be targeted in preventive and rehabilitative strategies for athletes.
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be addressed in this research.
Funding
This research did not receive any grants from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed equally to preparing the article.
Conflicts of interest
The authors declared no conflict of interest.
Type of Study: Research |
Subject:
Special
Received: 2025/09/27 | Accepted: 2025/10/30 | Published: 2025/11/1
Received: 2025/09/27 | Accepted: 2025/10/30 | Published: 2025/11/1
References
1. Hassabis D, Kumaran D, Summerfield C, Botvinick M. Neuroscience-inspired artificial intelligence. Neuron. 2017;95(2):245-58. [DOI:10.1016/j.neuron.2017.06.011] [PMID]
2. LeCun Y, Bengio Y, Hinton G. Deep learning. Nature. 2015;521(7553):436-44. [DOI:10.1038/nature14539] [PMID]
3. Haataamee F, Shojaodin SS. The Effect of Balance and Combined Exercises on Pain and Functional Characteristics of Female Athletes With Chronic Ankle Instability. Journal of Sport Biomechanics. 2019;4(4):28-41. [DOI:10.32598/biomechanics.4.4.28]
4. Doherty C, Bleakley C, Hertel J, Caulfield B, Ryan J, Delahunt E. Recovery from a first-time lateral ankle sprain and the predictors of chronic ankle instability: a prospective cohort analysis. The American Journal of Sports Medicine. 2016;44(4):995-1003. [DOI:10.1177/0363546516628870] [PMID]
5. Hertel J, Corbett RO. An updated model of chronic ankle instability. Journal of Athletic Training. 2019;54(6):572-88. [DOI:10.4085/1062-6050-344-18] [PMID]
6. Gribble PA, Delahunt E, Bleakley C, Caulfield B, Docherty C, Fourchet F, et al. Selection criteria for patients with chronic ankle instability in controlled research: a position statement of the International Ankle Consortium. Journal of Orthopaedic & Sports Physical Therapy. 2013;43(8):585-91. [DOI:10.2519/jospt.2013.0303] [PMID]
7. Claudino JG, Capanema DdO, de Souza TV, Serrão JC, Machado Pereira AC, Nassis GP. Current approaches to the use of artificial intelligence for injury risk assessment and performance prediction in team sports: a systematic review. Sports Medicine-Open. 2019;5(1):28. [DOI:10.1186/s40798-019-0202-3] [PMID]
8. Kaminski TW, Needle AR, Delahunt E. Prevention of lateral ankle sprains. Journal of Athletic Training. 2019;54(6):650-61. [DOI:10.4085/1062-6050-487-17] [PMID]
9. Fong DT, Chan Y-Y, Mok K-M, Yung PS, Chan K-M. Understanding acute ankle ligamentous sprain injury in sports. BMC Sports Science, Medicine and Rehabilitation. 2009;1(1):14. [DOI:10.1186/1758-2555-1-14] [PMID]
10. Rossi A, Pappalardo L, Cintia P, Iaia FM, Fernández J, Medina D. Effective injury forecasting in soccer with GPS training data and machine learning. PloS One. 2018;13(7):e0201264. [DOI:10.1371/journal.pone.0201264] [PMID]
11. Ulijaszek SJ, Kerr DA. Anthropometric measurement error and the assessment of nutritional status. British Journal of Nutrition. 1999;82(3):165-77. [DOI:10.1017/S0007114599001348] [PMID]
12. Bosy-Westphal A, Schautz B, Later W, Kehayias J, Gallagher D, Müller M. What makes a BIA equation unique? Validity of eight-electrode multifrequency BIA to estimate body composition in a healthy adult population. European Journal of Clinical Nutrition. 2013;67(1):S14-S21. [DOI:10.1038/ejcn.2012.160] [PMID]
13. Wang Y, Mei Q, Jiang H, Hollander K, Van den Berghe P, Fernandez J, et al. The Biomechanical Influence of Step Width on Typical Locomotor Activities: A Systematic Review. Sports Medicine-Open. 2024;10(1):83. [DOI:10.1186/s40798-024-00750-4] [PMID]
14. Menz HB. Alternative techniques for the clinical assessment of foot pronation. Journal of the American Podiatric Medical Association. 1998;88(3):119-29. [DOI:10.7547/87507315-88-3-119] [PMID]
15. Konor MM, Morton S, Eckerson JM, Grindstaff TL. Reliability of three measures of ankle dorsiflexion range of motion. International Journal of Sports Physical Therapy. 2012;7(3):279.
16. Rome K, Brown C. Randomized clinical trial into the impact of rigid foot orthoses on balance parameters in excessively pronated feet. Clinical Rehabilitation. 2004;18(6):624-30. [DOI:10.1191/0269215504cr767oa] [PMID]
17. Youdas JW, Bogard CL, Suman VJ. Reliability of goniometric measurements and visual estimates of ankle joint active range of motion obtained in a clinical setting. Archives of Physical Medicine and Rehabilitation. 1993;74(10):1113-8. [DOI:10.1016/0003-9993(93)90071-H] [PMID]
18. Bell DR, Guskiewicz KM, Clark MA, Padua DA. Systematic review of the balance error scoring system. Sports Health. 2011;3(3):287-95. [DOI:10.1177/1941738111403122] [PMID]
19. Springer BA, Marin R, Cyhan T, Roberts H, Gill NW. Normative values for the unipedal stance test with eyes open and closed. Journal of Geriatric Physical Therapy. 2007;30(1):8-15. [DOI:10.1519/00139143-200704000-00003] [PMID]
20. Raya MA, Gailey RS, Gaunaurd IA, Jayne DM, Campbell SM, Gagne E, et al. Comparison of three agility tests with male servicemembers: Edgren Side Step Test, T-Test, and Illinois Agility Test. Journal of Rehabilitation Research & Development. 2013;50(7): 951-960. [DOI:10.1682/JRRD.2012.05.0096] [PMID]
21. Waterman BR, Belmont PJ, Cameron KL, DeBerardino TM, Owens BD. Epidemiology of ankle sprain at the United States Military Academy. The American Journal of Sports Medicine. 2010;38(4):797-803. [DOI:10.1177/0363546509350757] [PMID]
22. Silva AJ, Costa AM, Oliveira PM, Reis VM, Saavedra J, Perl J, et al. The use of neural network technology to model swimming performance. Journal of Sports Science & Medicine. 2007;6(1):117.
23. Milgrom C, Shlamkovitch N, Finestone A, Eldad A, Laor A, Danon YL, et al. Risk factors for lateral ankle sprain: a prospective study among military recruits. Foot & ankle. 1991;12(1):26-30. [DOI:10.1177/107110079101200105] [PMID]
24. Guan Y. Why Do Humans Twist Their Ankle: A Nonlinear Dynamical Stability Model for Lower Limb. arXiv preprint arXiv:230503140. 2023.
25. Maeda N, Ikuta Y, Tsutsumi S, Arima S, Ishihara H, Ushio K, et al. Relationship of chronic ankle instability with foot alignment and dynamic postural stability in adolescent competitive athletes. Orthopaedic Journal of Sports Medicine. 2023;11(10):23259671231202220. [DOI:10.1177/23259671231202220] [PMID]
26. Martin RL, Davenport TE, Paulseth S, Wukich DK, Godges JJ, Altman RD, et al. Ankle stability and movement coordination impairments: ankle ligament sprains: clinical practice guidelines linked to the international classification of functioning, disability and health from the orthopaedic section of the American Physical Therapy Association. Journal of Orthopaedic & Sports Physical Therapy. 2013;43(9):A1-A40. [DOI:10.2519/jospt.2013.0305] [PMID]
27. Vomacka MM, Calhoun MR, Lininger MR, Ko J. Dorsiflexion range of motion in copers and those with chronic ankle instability. International Journal of Exercise Science. 2019;12(1):614. [DOI:10.70252/QLDK8340] [PMID]
28. Hubbard TJ, Kramer LC, Denegar CR, Hertel J. Contributing factors to chronic ankle instability. Foot & Ankle International. 2007;28(3):343-54. [DOI:10.3113/FAI.2007.0343] [PMID]
29. Sarvestan J, Svoboda Z. Acute effect of ankle kinesio and athletic taping on ankle range of motion during various agility tests in athletes with chronic ankle sprain. Journal of Sport Rehabilitation. 2019;29(5):527-32. [DOI:10.1123/jsr.2018-0398] [PMID]
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Journal of Sport Biomechanics
Department of Sport Biomechanics, Faculty of Humanities, Islamic Azad University, Hamedan Branch, Prof. Mousivand Blvd, Imam Khomeini Blvd, Hamedan, Iran.
Journal Tel: +98 81 34494042
Website: http://biomechanics.iauh.ac.ir
Email: sportbiomechanics@iauh.ac.ir
