

Volume 12, Issue 3 (11-2026)
J Sport Biomech 2026, 12(3): 394-404 |
Back to browse issues page


![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Elhami M, Yazdani S, Eskandar Nezhad M. Comparative Analysis of Dual-Task Effects on EMG Activity During Walking in Individuals with Hemiplegic Cerebral Palsy and Healthy Controls. J Sport Biomech 2026; 12 (3) :394-404
URL: http://biomechanics.iauh.ac.ir/article-1-471-en.html
URL: http://biomechanics.iauh.ac.ir/article-1-471-en.html



1- Department of Motor Behavior, Faculty of Physical Education and Sports Sciences, University of Tabriz, Tabriz, Iran.
Full-Text [PDF 964 kb]
(32 Downloads)
| Abstract (HTML) (95 Views)

Full-Text: (20 Views)
1. Introduction
The study of human movement and locomotion, particularly within dual-task paradigms, is of great importance in the fields of motor control and sports biomechanics. Walking is a low-impact, energy-efficient motor activity that serves as a primary mode of human transportation. It requires coordinated movements of the arms, legs, and trunk and is characterized by a repetitive bipedal pattern that propels the body forward in a controlled and efficient manner (1). As a fundamental and complex motor activity, walking relies on the seamless integration of cognitive, motor, and visual systems (2). In healthy individuals, this integration occurs automatically and efficiently; however, in populations with neurological impairments such as hemiplegic cerebral palsy (CP), this process is significantly disrupted.
Cerebral palsy (CP) is the most common motor disorder in childhood, with an incidence of approximately 1 per 1,000 live births in Europe (3). One-third of individuals with CP present with unilateral motor deficits (hemiplegic cerebral palsy), which represents the most common subtype observed at birth (4). Hemiplegic CP presents unique challenges in gait mechanics, balance control, and the execution of dual-task activities. These individuals commonly exhibit spasticity, muscle weakness, and impaired coordination, leading to frequent falls due to poor postural control and compromised dynamic balance (5), as well as altered gait patterns, reduced walking speed, shorter step lengths, increased step width (6, 7), and poor gait stability (8). Furthermore, more than 65% of children with CP demonstrate functional deficits in visuospatial processing, attention, and learning, along with altered activation of the sensorimotor cortex, impaired sensory white matter connectivity, and reduced performance on clinical sensory assessments (9, 10), all of which further exacerbate difficulties in performing dual-task activities.
Dual-task paradigms, which involve the simultaneous execution of a motor task and a cognitive or visual task, impose additional demands on the sensory and motor systems in this population (11). Compared with normal walking, dual-task walking further alters spatiotemporal gait parameters such as speed, step width, and step length in individuals with CP, leading to greater deterioration in gait performance and balance and requiring increased effort to maintain stability (11). Children with CP who experience deficits in executive functions, such as maintaining and dividing attention (7), face increased sensory-proprioceptive demands during dual-task conditions, including cognitive-motor and visual-motor tasks (12).
Motor impairments in CP, including reduced walking speed and shorter step length, are closely associated with abnormal somatosensory cortical activity (10). Moreover, excessive reliance on visual input during standing is linked to abnormal balance strategies (13) and an increased risk of delays in postural control, spatial awareness, and motor development (14). Visual input plays a critical role in maintaining postural stability in individuals with CP (15). Due to impairments in somatosensory and proprioceptive processing, these individuals often rely more heavily on visual cues than proprioceptive feedback during both upper- and lower-limb movements and during standing tasks (15, 16). The visual system is also essential for maintaining stability and planning movement trajectories during locomotion (17). In motor execution contexts, cognitive and attentional training tailored to specific motor tasks may optimize the use of visual information during skill performance. Overall, the combination of sensory deficits, abnormal cortical activation patterns, overreliance on vision, and motor limitations in CP contributes to inefficient motor planning and execution during dual-task conditions (10, 13), resulting in greater difficulty in performing simultaneous tasks due to competition for limited cognitive resources (7).
However, dual-task training during walking has shown promise in reducing secondary complications associated with functional decline and improving overall motor outcomes in this population. Previous studies across different populations have demonstrated that dual-task training can improve balance and gait quality in individuals with CP (11, 18). Moreover, such interventions have been shown to enhance gait mechanics and balance in this population (19, 20). Despite these findings, the underlying mechanisms of these improvements and the specific neuromuscular responses of different muscles under various dual-task conditions (cognitive, motor, and visual) remain poorly understood. This gap in knowledge limits the development of optimized rehabilitation protocols tailored to individuals with hemiplegic CP.
Electromyographic (EMG) analysis provides a powerful method for investigating neuromuscular adaptations and compensatory strategies during walking under dual-task conditions. A deeper understanding of muscle activation patterns in selected lower-limb and trunk muscles during dual-task performance can provide valuable insight into the mechanisms underlying gait disturbances and balance impairments in individuals with hemiplegic CP and help identify potential targets for therapeutic intervention. Therefore, the present study aimed to investigate the effects of different dual-task conditions on the electromyographic activity of selected lower-limb and trunk muscles during walking in individuals with hemiplegic CP compared with healthy controls. This research contributes to the understanding of motor control in hemiplegic CP and provides a foundation for evidence-based rehabilitation strategies aimed at improving functional mobility and quality of life in this population.
2. Methods
2.1. Participants
The study population comprised individuals diagnosed with left-sided hemiplegic cerebral palsy in Tabriz, Iran. From this population, 12 participants were voluntarily selected as the statistical sample. Additionally, 12 healthy age-, height-, and weight-matched individuals were recruited as the control group. Table 1 summarizes the mean age, height, weight, and body mass index (BMI) of participants in both groups. Prior to participation, the study protocol was fully explained to all participants and their parents, and written informed consent was obtained to ensure voluntary participation. The study was approved by the Ethics Committee of the University of Tabriz under the code IR.TABRIZU.REC.1399.005. The inclusion criteria for participants with cerebral palsy (CP) included left-sided unilateral cerebral palsy (21), the ability to understand and follow verbal instructions, independent walking ability, adequate balance control, the ability to carry a box, and the absence of significant cognitive impairments. The exclusion criteria included inability to control balance, inability to walk independently, lack of cooperation from parents or the child, cognitive impairment, intellectual disability, and visual or auditory problems. The control group consisted of healthy individuals with no history of surgery or neuromuscular, visual, auditory, or motor impairments.
The study of human movement and locomotion, particularly within dual-task paradigms, is of great importance in the fields of motor control and sports biomechanics. Walking is a low-impact, energy-efficient motor activity that serves as a primary mode of human transportation. It requires coordinated movements of the arms, legs, and trunk and is characterized by a repetitive bipedal pattern that propels the body forward in a controlled and efficient manner (1). As a fundamental and complex motor activity, walking relies on the seamless integration of cognitive, motor, and visual systems (2). In healthy individuals, this integration occurs automatically and efficiently; however, in populations with neurological impairments such as hemiplegic cerebral palsy (CP), this process is significantly disrupted.
Cerebral palsy (CP) is the most common motor disorder in childhood, with an incidence of approximately 1 per 1,000 live births in Europe (3). One-third of individuals with CP present with unilateral motor deficits (hemiplegic cerebral palsy), which represents the most common subtype observed at birth (4). Hemiplegic CP presents unique challenges in gait mechanics, balance control, and the execution of dual-task activities. These individuals commonly exhibit spasticity, muscle weakness, and impaired coordination, leading to frequent falls due to poor postural control and compromised dynamic balance (5), as well as altered gait patterns, reduced walking speed, shorter step lengths, increased step width (6, 7), and poor gait stability (8). Furthermore, more than 65% of children with CP demonstrate functional deficits in visuospatial processing, attention, and learning, along with altered activation of the sensorimotor cortex, impaired sensory white matter connectivity, and reduced performance on clinical sensory assessments (9, 10), all of which further exacerbate difficulties in performing dual-task activities.
Dual-task paradigms, which involve the simultaneous execution of a motor task and a cognitive or visual task, impose additional demands on the sensory and motor systems in this population (11). Compared with normal walking, dual-task walking further alters spatiotemporal gait parameters such as speed, step width, and step length in individuals with CP, leading to greater deterioration in gait performance and balance and requiring increased effort to maintain stability (11). Children with CP who experience deficits in executive functions, such as maintaining and dividing attention (7), face increased sensory-proprioceptive demands during dual-task conditions, including cognitive-motor and visual-motor tasks (12).
Motor impairments in CP, including reduced walking speed and shorter step length, are closely associated with abnormal somatosensory cortical activity (10). Moreover, excessive reliance on visual input during standing is linked to abnormal balance strategies (13) and an increased risk of delays in postural control, spatial awareness, and motor development (14). Visual input plays a critical role in maintaining postural stability in individuals with CP (15). Due to impairments in somatosensory and proprioceptive processing, these individuals often rely more heavily on visual cues than proprioceptive feedback during both upper- and lower-limb movements and during standing tasks (15, 16). The visual system is also essential for maintaining stability and planning movement trajectories during locomotion (17). In motor execution contexts, cognitive and attentional training tailored to specific motor tasks may optimize the use of visual information during skill performance. Overall, the combination of sensory deficits, abnormal cortical activation patterns, overreliance on vision, and motor limitations in CP contributes to inefficient motor planning and execution during dual-task conditions (10, 13), resulting in greater difficulty in performing simultaneous tasks due to competition for limited cognitive resources (7).
However, dual-task training during walking has shown promise in reducing secondary complications associated with functional decline and improving overall motor outcomes in this population. Previous studies across different populations have demonstrated that dual-task training can improve balance and gait quality in individuals with CP (11, 18). Moreover, such interventions have been shown to enhance gait mechanics and balance in this population (19, 20). Despite these findings, the underlying mechanisms of these improvements and the specific neuromuscular responses of different muscles under various dual-task conditions (cognitive, motor, and visual) remain poorly understood. This gap in knowledge limits the development of optimized rehabilitation protocols tailored to individuals with hemiplegic CP.
Electromyographic (EMG) analysis provides a powerful method for investigating neuromuscular adaptations and compensatory strategies during walking under dual-task conditions. A deeper understanding of muscle activation patterns in selected lower-limb and trunk muscles during dual-task performance can provide valuable insight into the mechanisms underlying gait disturbances and balance impairments in individuals with hemiplegic CP and help identify potential targets for therapeutic intervention. Therefore, the present study aimed to investigate the effects of different dual-task conditions on the electromyographic activity of selected lower-limb and trunk muscles during walking in individuals with hemiplegic CP compared with healthy controls. This research contributes to the understanding of motor control in hemiplegic CP and provides a foundation for evidence-based rehabilitation strategies aimed at improving functional mobility and quality of life in this population.
2. Methods
2.1. Participants
The study population comprised individuals diagnosed with left-sided hemiplegic cerebral palsy in Tabriz, Iran. From this population, 12 participants were voluntarily selected as the statistical sample. Additionally, 12 healthy age-, height-, and weight-matched individuals were recruited as the control group. Table 1 summarizes the mean age, height, weight, and body mass index (BMI) of participants in both groups. Prior to participation, the study protocol was fully explained to all participants and their parents, and written informed consent was obtained to ensure voluntary participation. The study was approved by the Ethics Committee of the University of Tabriz under the code IR.TABRIZU.REC.1399.005. The inclusion criteria for participants with cerebral palsy (CP) included left-sided unilateral cerebral palsy (21), the ability to understand and follow verbal instructions, independent walking ability, adequate balance control, the ability to carry a box, and the absence of significant cognitive impairments. The exclusion criteria included inability to control balance, inability to walk independently, lack of cooperation from parents or the child, cognitive impairment, intellectual disability, and visual or auditory problems. The control group consisted of healthy individuals with no history of surgery or neuromuscular, visual, auditory, or motor impairments.
2.2. Electromyography (EMG) Setup
Surface electromyography (EMG) recordings were obtained from the erector spinae (L3), biceps femoris (BF), and rectus femoris (RF) muscles using a USB2+ EMG system (manufactured in Italy) with a sampling frequency of 1000 Hz. Bipolar gel surface electrodes with an inter-electrode distance of 1.7 cm were used. Prior to electrode placement, the skin was prepared according to the SENIAM European protocol, which included shaving the electrode sites, cleaning the skin with alcohol, and removing dead epithelial cells to reduce impedance. Electrodes were placed parallel to the muscle fiber orientation following standard SENIAM guidelines. For the erector spinae muscle at the L3 level, electrodes were placed 3 cm lateral to the spinous process of the third lumbar vertebra (22). For the rectus femoris (RF), electrodes were positioned at the midpoint between the anterior superior iliac spine and the patella (23). For the biceps femoris (BF), electrodes were placed at the midpoint between the ischial tuberosity and the lateral femoral condyle (24). All procedures followed the SENIAM European recommendations (25).
2.3. Experimental Procedure
After electrode placement, all electrodes were secured using hypoallergenic tape and bandages to minimize movement artifacts. Cables were bundled and fixed to the body to further reduce noise. Electrodes were placed bilaterally, and a reference electrode was attached to the wrist. Participants performed walking trials along a 10-meter walkway under three conditions: motor, cognitive, and visual dual-task conditions. Each condition was repeated six times, and a foot switch was used to determine gait cycles. In the motor task condition, participants carried a box corresponding to 10% of their body weight. In the cognitive task condition, participants performed backward counting from 20 to 0 while verbalizing even numbers (20, 18, 16, etc.) (26). In the visual task condition, markers were placed at fixed intervals along the walkway, and participants were instructed to step on these markers while walking. Following the walking trials, maximal voluntary isometric contractions (MVIC) were recorded for the L3, RF, and BF muscles for EMG normalization. The erector spinae MVIC was assessed in the Sorensen position, in which participants lay prone with the upper body extended beyond the edge of the table at hip level while the lower limbs were secured. Participants were instructed to maintain a zero-degree trunk extension while resisting applied force (22, 27).
The rectus femoris MVIC was performed in a seated position with the knee secured, and participants were instructed to perform maximal knee extension against resistance at 90° hip flexion (24). The biceps femoris MVIC was assessed in a prone position with the pelvis and thighs stabilized, while participants performed maximal knee flexion against external resistance (28).
2.4. Data Processing and Statistical Analysis
Electromyographic signals were processed using OT BioLab software. Signals were filtered using a 10–350 Hz band-pass filter and a 50 Hz notch filter. Root mean square (RMS) values were extracted for analysis. For normalization, RMS values obtained during walking tasks were divided by RMS values obtained during MVIC for each corresponding muscle and expressed as a percentage. Statistical analysis was performed using SPSS version 22. Descriptive and inferential statistics were applied. The Shapiro–Wilk test was used to assess normality. Between-group and within-group comparisons were performed using ANOVA and repeated-measures ANOVA. Statistical significance was set at p ≤ 0.05.
3. Results
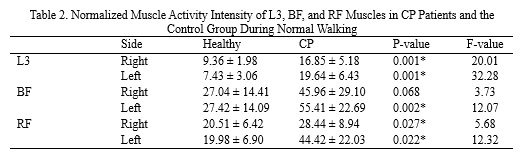
Table 2 presents the normalized muscle activity intensity for the L3, BF, and RF muscles in individuals with cerebral palsy (CP) and the control group during normal walking. The results indicate that during normal walking, the electrical activity intensity of the RF and L3 muscles on the right side of CP patients was significantly higher than that of healthy individuals (p = 0.027 and p = 0.001, respectively). On the left side of the body, the normalized electrical activity intensity of the L3, BF, and RF muscles in CP patients was approximately 2.48, 1.88, and 2.47 times higher than that of healthy individuals, respectively (p = 0.001, p = 0.002, and p = 0.022).
Surface electromyography (EMG) recordings were obtained from the erector spinae (L3), biceps femoris (BF), and rectus femoris (RF) muscles using a USB2+ EMG system (manufactured in Italy) with a sampling frequency of 1000 Hz. Bipolar gel surface electrodes with an inter-electrode distance of 1.7 cm were used. Prior to electrode placement, the skin was prepared according to the SENIAM European protocol, which included shaving the electrode sites, cleaning the skin with alcohol, and removing dead epithelial cells to reduce impedance. Electrodes were placed parallel to the muscle fiber orientation following standard SENIAM guidelines. For the erector spinae muscle at the L3 level, electrodes were placed 3 cm lateral to the spinous process of the third lumbar vertebra (22). For the rectus femoris (RF), electrodes were positioned at the midpoint between the anterior superior iliac spine and the patella (23). For the biceps femoris (BF), electrodes were placed at the midpoint between the ischial tuberosity and the lateral femoral condyle (24). All procedures followed the SENIAM European recommendations (25).
2.3. Experimental Procedure
After electrode placement, all electrodes were secured using hypoallergenic tape and bandages to minimize movement artifacts. Cables were bundled and fixed to the body to further reduce noise. Electrodes were placed bilaterally, and a reference electrode was attached to the wrist. Participants performed walking trials along a 10-meter walkway under three conditions: motor, cognitive, and visual dual-task conditions. Each condition was repeated six times, and a foot switch was used to determine gait cycles. In the motor task condition, participants carried a box corresponding to 10% of their body weight. In the cognitive task condition, participants performed backward counting from 20 to 0 while verbalizing even numbers (20, 18, 16, etc.) (26). In the visual task condition, markers were placed at fixed intervals along the walkway, and participants were instructed to step on these markers while walking. Following the walking trials, maximal voluntary isometric contractions (MVIC) were recorded for the L3, RF, and BF muscles for EMG normalization. The erector spinae MVIC was assessed in the Sorensen position, in which participants lay prone with the upper body extended beyond the edge of the table at hip level while the lower limbs were secured. Participants were instructed to maintain a zero-degree trunk extension while resisting applied force (22, 27).
The rectus femoris MVIC was performed in a seated position with the knee secured, and participants were instructed to perform maximal knee extension against resistance at 90° hip flexion (24). The biceps femoris MVIC was assessed in a prone position with the pelvis and thighs stabilized, while participants performed maximal knee flexion against external resistance (28).
2.4. Data Processing and Statistical Analysis
Electromyographic signals were processed using OT BioLab software. Signals were filtered using a 10–350 Hz band-pass filter and a 50 Hz notch filter. Root mean square (RMS) values were extracted for analysis. For normalization, RMS values obtained during walking tasks were divided by RMS values obtained during MVIC for each corresponding muscle and expressed as a percentage. Statistical analysis was performed using SPSS version 22. Descriptive and inferential statistics were applied. The Shapiro–Wilk test was used to assess normality. Between-group and within-group comparisons were performed using ANOVA and repeated-measures ANOVA. Statistical significance was set at p ≤ 0.05.
3. Results
Table 2 presents the normalized muscle activity intensity for the L3, BF, and RF muscles in individuals with cerebral palsy (CP) and the control group during normal walking. The results indicate that during normal walking, the electrical activity intensity of the RF and L3 muscles on the right side of CP patients was significantly higher than that of healthy individuals (p = 0.027 and p = 0.001, respectively). On the left side of the body, the normalized electrical activity intensity of the L3, BF, and RF muscles in CP patients was approximately 2.48, 1.88, and 2.47 times higher than that of healthy individuals, respectively (p = 0.001, p = 0.002, and p = 0.022).
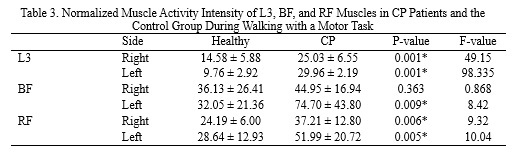
Table 3 summarizes the normalized muscle activity intensity of the L3, BF, and RF muscles in CP patients and the control group during walking with a dual task. The results indicated that during walking with a dual task, the activity intensity of the L3 and RF muscles on the right side of CP patients was approximately 1.54 and 1.65 times higher than that of healthy individuals (p = 0.001 and p = 0.006, respectively). Furthermore, during walking with a dual task, the activity intensity of the L3, BF, and RF muscles on the left side of CP patients was approximately 2.53, 2.21, and 1.74 times higher than that of healthy individuals, respectively (p = 0.001, p = 0.009, and p = 0.005).
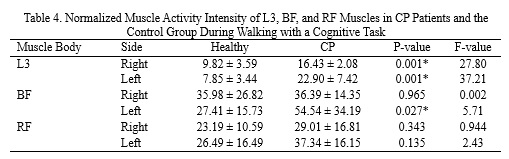
Table 4 displays the normalized muscle activity intensity of the L3, BF, and RF muscles in CP patients and the control group during walking with a dual cognitive task. The activity intensity of the L3 muscle on the right side of CP patients was approximately 1.38 times higher than that of healthy individuals. Additionally, the activity intensity of the L3 and BF muscles on the left side of CP patients was significantly higher than that of healthy individuals (p = 0.001 and p = 0.027, respectively).
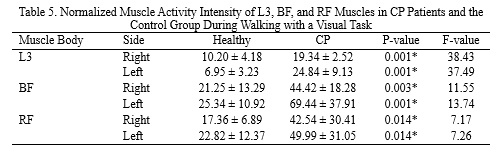
Table 5 presents the normalized muscle activity intensity of the L3, BF, and RF muscles in CP patients and the control group during walking with a dual visual task. The activity intensity of the L3 and BF muscles on the right side of CP patients was approximately 1.52 and 1.81 times higher than that of healthy individuals. Moreover, the activity intensity of the L3, BF, and RF muscles on the left side of CP patients was significantly higher than that of healthy individuals (p = 0.001, p = 0.001, and p = 0.014, respectively).
The effect of the type of dual task on the muscle activity intensity differed between the CP and healthy groups. The cognitive and visual dual tasks had a greater impact on the CP group compared to the healthy group. As illustrated in Fig. 1, there was a significant interaction between the group and the motor task (p = 0.001). Additionally, the pattern of changes in muscle activity intensity varied between the healthy and CP groups across different muscles during various dual tasks (Fig. 2). A significant interaction was observed among the three factors of muscle, group, and dual tasks (p = 0.020). Furthermore, the motor tasks had a differential effect on the activity intensity of the L3, BF, and RF muscles in the healthy and CP groups (p = 0.001). Based on the results of the factor analysis (Fig. 3), it was found that the effect of body side differed between the two groups (p = 0.010), with which the left side of CP patients experiencing more tension than the right side (p = 0.002).
4. Discussion
The aim of this study was to investigate the effects of motor, cognitive, and visual dual-task conditions on the EMG activity of the L3, BF, and RF muscles during walking. The results showed that, except for normal walking and the motor dual-task condition where no significant difference was observed in the right BF muscle, muscle activity in both right and left L3, BF, and RF muscles was significantly higher in individuals with CP compared to healthy controls across all conditions.
These findings are consistent with previous studies (29–32), which also reported increased EMG activity during walking in individuals with cerebral palsy. Similarly, higher electrical activity of the internal and external oblique muscles at rest has also been reported in this population (33). Prior research has demonstrated that individuals with CP exhibit impaired balance control, greater postural sway, reduced postural stability, and altered motor control strategies compared to healthy individuals (34). In addition, gait impairments such as reduced walking speed, shorter step length, increased step width, decreased hip range of motion, and increased double-support time have been widely documented (35), along with reduced gait stability (8, 34). Therefore, higher muscle activation in CP may reflect a compensatory mechanism required to maintain postural stability in both static and dynamic conditions. Furthermore, muscle weakness commonly observed in this population (36) may further contribute to increased recruitment of motor units during walking as a compensatory strategy, resulting in elevated EMG activity. Overall, the increased muscle activation observed in individuals with CP compared with healthy controls may be attributed to both compensatory demands for postural control and neuromuscular inefficiency associated with muscle weakness.
A more detailed analysis of the results revealed that L3 muscle activity was higher in individuals with CP than in healthy controls. This increased activation of the lumbar erector spinae at the L3 level may be related to greater pelvic rotation observed in individuals with CP. Previous kinematic studies have reported increased pelvic rotation during walking in individuals with CP compared to typically developing peers (37). Consequently, increased pelvic motion may alter spinal kinematics, thereby requiring greater activation of the L3 musculature to maintain trunk stability during gait.
Similarly, RF muscle activity was higher in individuals with CP. Previous studies have reported knee instability and collapse in this population (34). Increased activation of the rectus femoris may therefore represent a compensatory strategy to stabilize the knee joint and reduce the risk of collapse during walking (38). In addition, BF muscle activity was also higher in individuals with CP compared with healthy controls. The biceps femoris plays an important role in controlling hip flexion and extension through eccentric and concentric actions (39). Given the presence of hip instability and altered gait mechanics in CP (35), increased BF activity may function as a compensatory mechanism to prevent hip collapse. Moreover, due to the flexed hip posture commonly observed in this population (38), greater force production is required for hip extension, which is associated with increased activation of hip extensors such as the biceps femoris. Additionally, increased muscle tone due to spasticity in the affected limbs may further contribute to elevated EMG activity (40).
According to the findings of the present study, muscle activation during motor and visual dual-task walking was higher than during cognitive dual-task and single-task walking in individuals with CP. Individuals with cerebral palsy have impairments in processing somatosensory and proprioceptive information and therefore rely more heavily on visual input than proprioception during motor tasks, including walking. Previous research has also shown that individuals with CP rely more on visual information for gait control compared with healthy individuals (21). In addition, visual tasks have been reported to negatively affect postural balance (2). Sharma (11) also demonstrated that during visual dual-task conditions compared with simple walking or auditory and cognitive dual tasks, individuals with CP exhibited increased gait speed, step length, and step width. These alterations in spatiotemporal parameters may influence muscle activation patterns and contribute to the increased EMG activity observed in the present study.
During motor dual-task conditions, such as walking while carrying a load, both tasks compete for attentional resources, leading to further disruption of balance control. As a result, individuals must exert greater effort to maintain stability and recruit additional sensory-proprioceptive mechanisms. It has been suggested that dual-task performance reduces attentional capacity and induces interference effects (41, 42), resulting in a higher cognitive-motor cost compared with healthy individuals (43). This supports the notion that attentional resources and cortical control mechanisms are required to compensate for gait impairments in individuals with CP (44). The present findings are also consistent with those of Yazdani (45) and Hung (46), who reported increased muscle activity during load carriage conditions.
The results further indicated asymmetrical muscle activation patterns between the affected and non-affected sides in individuals with hemiplegic CP, with higher activation observed on the affected (left) side. Since participants presented with left-sided hemiplegia, increased muscle tone and neuromuscular activity on the affected side may explain this asymmetry. This finding is supported by Franz and Meeuwsen, who reported that interhemispheric transfer via the corpus callosum, which contributes to interlimb coordination, is altered in individuals with hemiplegia and affects limb symmetry (47). Additionally, previous research has shown that muscle activation patterns in individuals with CP are highly individualized and that kinematic abnormalities are not always directly proportional to muscle activation patterns (48). However, these findings are in contrast with those of Kulmala (49), who reported no significant differences in ankle and knee extensor activity between affected and unaffected limbs during walking.
This study has several limitations. Ground reaction forces and joint kinetics were not assessed. Future studies should investigate kinetic variables during dual-task walking to provide a more comprehensive understanding of gait mechanics in individuals with CP. Furthermore, the present study focused exclusively on muscle activation patterns in individuals with hemiplegic CP; therefore, the findings cannot be generalized to other populations or functional tasks.
5. Conclusion
The results of this study indicate that individuals with cerebral palsy exhibit greater muscle activity during walking compared with healthy individuals. This increased muscle activity appears to reflect a compensatory strategy to maintain balance and postural control, as well as to offset underlying muscle weakness. Furthermore, both motor and visual dual-task conditions increased the activity of the investigated muscles in both groups. These findings suggest that dual-task paradigms impose additional neuromuscular demands during walking. Accordingly, incorporating dual-task-based exercises may help enhance neuromuscular activation in individuals with cerebral palsy and contribute to improvements in motor function and divided attention. Therefore, dual-task conditions should be considered when assessing gait and when designing rehabilitation and exercise programs for individuals with cerebral palsy.
Ethical Considerations
Compliance with ethical guidelines
This study was conducted in accordance with the ethical standards of the institutional and/or national research committee and with the principles of the Declaration of Helsinki. All participants voluntarily took part in the study and provided written informed consent prior to enrollment. The study protocol was approved by the Ethics Committee of the University of Tabriz under the code IR.TABRIZU.REC.1399.005.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors' contributions
All authors contributed to the conceptualization, data collection, analysis, and preparation of the manuscript. All authors have read and approved the final version of the manuscript.
Conflicts of interest
The authors declare that they have no conflicts of interest.
4. Discussion
The aim of this study was to investigate the effects of motor, cognitive, and visual dual-task conditions on the EMG activity of the L3, BF, and RF muscles during walking. The results showed that, except for normal walking and the motor dual-task condition where no significant difference was observed in the right BF muscle, muscle activity in both right and left L3, BF, and RF muscles was significantly higher in individuals with CP compared to healthy controls across all conditions.
These findings are consistent with previous studies (29–32), which also reported increased EMG activity during walking in individuals with cerebral palsy. Similarly, higher electrical activity of the internal and external oblique muscles at rest has also been reported in this population (33). Prior research has demonstrated that individuals with CP exhibit impaired balance control, greater postural sway, reduced postural stability, and altered motor control strategies compared to healthy individuals (34). In addition, gait impairments such as reduced walking speed, shorter step length, increased step width, decreased hip range of motion, and increased double-support time have been widely documented (35), along with reduced gait stability (8, 34). Therefore, higher muscle activation in CP may reflect a compensatory mechanism required to maintain postural stability in both static and dynamic conditions. Furthermore, muscle weakness commonly observed in this population (36) may further contribute to increased recruitment of motor units during walking as a compensatory strategy, resulting in elevated EMG activity. Overall, the increased muscle activation observed in individuals with CP compared with healthy controls may be attributed to both compensatory demands for postural control and neuromuscular inefficiency associated with muscle weakness.
A more detailed analysis of the results revealed that L3 muscle activity was higher in individuals with CP than in healthy controls. This increased activation of the lumbar erector spinae at the L3 level may be related to greater pelvic rotation observed in individuals with CP. Previous kinematic studies have reported increased pelvic rotation during walking in individuals with CP compared to typically developing peers (37). Consequently, increased pelvic motion may alter spinal kinematics, thereby requiring greater activation of the L3 musculature to maintain trunk stability during gait.
Similarly, RF muscle activity was higher in individuals with CP. Previous studies have reported knee instability and collapse in this population (34). Increased activation of the rectus femoris may therefore represent a compensatory strategy to stabilize the knee joint and reduce the risk of collapse during walking (38). In addition, BF muscle activity was also higher in individuals with CP compared with healthy controls. The biceps femoris plays an important role in controlling hip flexion and extension through eccentric and concentric actions (39). Given the presence of hip instability and altered gait mechanics in CP (35), increased BF activity may function as a compensatory mechanism to prevent hip collapse. Moreover, due to the flexed hip posture commonly observed in this population (38), greater force production is required for hip extension, which is associated with increased activation of hip extensors such as the biceps femoris. Additionally, increased muscle tone due to spasticity in the affected limbs may further contribute to elevated EMG activity (40).
According to the findings of the present study, muscle activation during motor and visual dual-task walking was higher than during cognitive dual-task and single-task walking in individuals with CP. Individuals with cerebral palsy have impairments in processing somatosensory and proprioceptive information and therefore rely more heavily on visual input than proprioception during motor tasks, including walking. Previous research has also shown that individuals with CP rely more on visual information for gait control compared with healthy individuals (21). In addition, visual tasks have been reported to negatively affect postural balance (2). Sharma (11) also demonstrated that during visual dual-task conditions compared with simple walking or auditory and cognitive dual tasks, individuals with CP exhibited increased gait speed, step length, and step width. These alterations in spatiotemporal parameters may influence muscle activation patterns and contribute to the increased EMG activity observed in the present study.
During motor dual-task conditions, such as walking while carrying a load, both tasks compete for attentional resources, leading to further disruption of balance control. As a result, individuals must exert greater effort to maintain stability and recruit additional sensory-proprioceptive mechanisms. It has been suggested that dual-task performance reduces attentional capacity and induces interference effects (41, 42), resulting in a higher cognitive-motor cost compared with healthy individuals (43). This supports the notion that attentional resources and cortical control mechanisms are required to compensate for gait impairments in individuals with CP (44). The present findings are also consistent with those of Yazdani (45) and Hung (46), who reported increased muscle activity during load carriage conditions.
The results further indicated asymmetrical muscle activation patterns between the affected and non-affected sides in individuals with hemiplegic CP, with higher activation observed on the affected (left) side. Since participants presented with left-sided hemiplegia, increased muscle tone and neuromuscular activity on the affected side may explain this asymmetry. This finding is supported by Franz and Meeuwsen, who reported that interhemispheric transfer via the corpus callosum, which contributes to interlimb coordination, is altered in individuals with hemiplegia and affects limb symmetry (47). Additionally, previous research has shown that muscle activation patterns in individuals with CP are highly individualized and that kinematic abnormalities are not always directly proportional to muscle activation patterns (48). However, these findings are in contrast with those of Kulmala (49), who reported no significant differences in ankle and knee extensor activity between affected and unaffected limbs during walking.
This study has several limitations. Ground reaction forces and joint kinetics were not assessed. Future studies should investigate kinetic variables during dual-task walking to provide a more comprehensive understanding of gait mechanics in individuals with CP. Furthermore, the present study focused exclusively on muscle activation patterns in individuals with hemiplegic CP; therefore, the findings cannot be generalized to other populations or functional tasks.
5. Conclusion
The results of this study indicate that individuals with cerebral palsy exhibit greater muscle activity during walking compared with healthy individuals. This increased muscle activity appears to reflect a compensatory strategy to maintain balance and postural control, as well as to offset underlying muscle weakness. Furthermore, both motor and visual dual-task conditions increased the activity of the investigated muscles in both groups. These findings suggest that dual-task paradigms impose additional neuromuscular demands during walking. Accordingly, incorporating dual-task-based exercises may help enhance neuromuscular activation in individuals with cerebral palsy and contribute to improvements in motor function and divided attention. Therefore, dual-task conditions should be considered when assessing gait and when designing rehabilitation and exercise programs for individuals with cerebral palsy.
Ethical Considerations
Compliance with ethical guidelines
This study was conducted in accordance with the ethical standards of the institutional and/or national research committee and with the principles of the Declaration of Helsinki. All participants voluntarily took part in the study and provided written informed consent prior to enrollment. The study protocol was approved by the Ethics Committee of the University of Tabriz under the code IR.TABRIZU.REC.1399.005.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors' contributions
All authors contributed to the conceptualization, data collection, analysis, and preparation of the manuscript. All authors have read and approved the final version of the manuscript.
Conflicts of interest
The authors declare that they have no conflicts of interest.
Type of Study: Research |
Subject:
Special
Received: 2025/11/23 | Accepted: 2026/06/16 | Published: 2026/06/18
Received: 2025/11/23 | Accepted: 2026/06/16 | Published: 2026/06/18
References
1. Winter DA. Biomechanics and motor control of human movement. Hoboken (NJ): John Wiley & Sons; 2009. [DOI:10.1002/9780470549148]
2. Carvalho JP, Bento-Torres J, da Silva DJ, et al. Cognitive and visual interactions in the decline of postural stability in healthy older adults. Brazilian Journal of Physical Therapy. 2024;28:100806. [DOI:10.1016/j.bjpt.2024.100806]
3. Stavsky M, Mor O, Mastrolia SA, Greenbaum S, Than NG, Erez O. Cerebral palsy-trends in epidemiology and recent development in prenatal mechanisms of disease, treatment, and prevention. Frontiers in Pediatrics. 2017;5:21. [DOI:10.3389/fped.2017.00021]
4. Kulak W, Sobaniec W. Comparisons of right and left hemiparetic cerebral palsy. Pediatric Neurology. 2004;31(2):101-108. [DOI:10.1016/j.pediatrneurol.2004.01.009]
5. Gordon AM, Charles J, Wolf SL. Efficacy of constraint-induced movement therapy on involved upper-extremity use in children with hemiplegic cerebral palsy is not age-dependent. Pediatrics. 2006;117(3):e363-e373. [DOI:10.1542/peds.2005-1009]
6. Galli M, Cimolin V, Rigoldi C, Tenore N, Albertini G. Gait patterns in hemiplegic children with cerebral palsy: comparison of right and left hemiplegia. Research in Developmental Disabilities. 2010;31(6):1340-1345. [DOI:10.1016/j.ridd.2010.07.007]
7. Carcreff L, Bonnefoy-Mazure A, Valenza N, Allali G, Fluss J, Armand S. Influence of cognitive-motor interference on gait spatiotemporal parameters in children and adolescents with cerebral palsy: a preliminary study. Gait & Posture. 2016;49:1-5. [DOI:10.1016/j.gaitpost.2016.07.084]
8. Cimolin V, Galli MA, Tenore NU, Albertini GI, Crivellini M. Gait strategy of uninvolved limb in children with spastic hemiplegia. European Journal of Physical and Rehabilitation Medicine. 2007;43(3):303-310.
9. Hoon AH Jr, Stashinko EE, Nagae LM, Lin DD, Keller J, Bastian AM, et al. Sensory and motor deficits in children with cerebral palsy born preterm correlate with diffusion tensor imaging abnormalities in thalamocortical pathways. Developmental Medicine & Child Neurology. 2009;51(9):697-704. [DOI:10.1111/j.1469-8749.2009.03306.x]
10. Kurz MJ, Heinrichs-Graham E, Becker KM, Wilson TW. The magnitude of somatosensory cortical activity is related to mobility and strength impairments in children with cerebral palsy. Journal of Neurophysiology. 2015;113(9):3143-3150. [DOI:10.1152/jn.00602.2014]
11. Sharma A, Saxena A, Thakur K. The effect of single and dual task on spatiotemporal gait parameters in children with spastic cerebral palsy. Journal of Society of Indian Physiotherapists. 2024;8(1):14-19. [DOI:10.4103/jsip.jsip_95_23]
12. Houwink A, Aarts PB, Geurts AC, Steenbergen B. A neurocognitive perspective on developmental disregard in children with hemiplegic cerebral palsy. Research in Developmental Disabilities. 2011;32(6):2157-2163. [DOI:10.1016/j.ridd.2011.07.012]
13. Yu Y, Tucker CA, Lauer RT, Keshner EA. Influence of visual dependence on intersegmental coordination during upright stance in cerebral palsy. Journal of Motor Behavior. 2020;52(3):249-261. [DOI:10.1080/00222895.2019.1610860]
14. Sonksen PM, Dale N. Visual impairment in infancy: impact on neurodevelopmental and neurobiological processes. Developmental Medicine & Child Neurology. 2002;44(11):782-791. [DOI:10.1111/j.1469-8749.2002.tb00287.x]
15. Lidbeck C, Bartonek Å, Yadav P, et al. The role of visual stimuli on standing posture in children with bilateral cerebral palsy. BMC Neurology. 2016;16:1-9. [DOI:10.1186/s12883-016-0676-2]
16. Sansare A, Reimann H, Bodt B, et al. Reliance on vision for walking balance is related to somatosensory deficits in individuals with cerebral palsy. medRxiv. 2024. [DOI:10.1101/2024.02.07.24302467]
17. Hallemans A, Ortibus E, Meire F, Aerts P. Low vision affects dynamic stability of gait. Gait & Posture. 2010;32(4):547-551. [DOI:10.1016/j.gaitpost.2010.07.018]
18. Afzal MT, Tariq S, Khan MS, et al. Effects of additional functional strength training on mobility in children with hemiplegic cerebral palsy. Rehabilitation Journal. 2023;7(4):14-19. [DOI:10.52567/trehabj.v7i04.8]
19. Uysal İ, Özden F, Tümtürk İ, İmerci A. The effectiveness of dual-task exercise training on balance, mobility, physical performance, and quality of life in children with cerebral palsy: a single-blind randomized controlled trial. Irish Journal of Medical Science. 2024;193(2):813-821. [DOI:10.1007/s11845-023-03530-3]
20. Hall JB, Chole D, Thomas J, Guess T. A novel multimodal platform detects gait and balance dual-task interference in unilateral cerebral palsy. Proceedings of the Combined Sections Meeting (CSM), USA; 2025.
21. Sansare A, Arcodia M, Lee SC, Jeka J, Reimann H. Individuals with cerebral palsy show altered responses to visual perturbations during walking. Frontiers in Human Neuroscience. 2022;16:977032. [DOI:10.3389/fnhum.2022.977032]
22. de Sèze MP, Cazalets JR. Anatomical optimization of skin electrode placement to record electromyographic activity of erector spinae muscles. Surgical and Radiologic Anatomy. 2008;30(2):137-143. [DOI:10.1007/s00276-007-0289-y]
23. Maffiuletti NA, Lepers R. Quadriceps femoris torque and EMG activity in seated versus supine position. Medicine & Science in Sports & Exercise. 2003;35(9):1511-1516. [DOI:10.1249/01.MSS.0000084426.03247.93]
24. Padulo J, Tiloca A, Powell D, et al. EMG amplitude of the biceps femoris during jumping compared to landing movements. SpringerPlus. 2013;2:1-7. [DOI:10.1186/2193-1801-2-520]
25. Hermens HJ, Freriks B, Disselhorst-Klug C, Rau G. Development of recommendations for SEMG sensors and sensor placement procedures. Journal of Electromyography and Kinesiology. 2000;10(5):361-375. [DOI:10.1016/S1050-6411(00)00027-4]
26. Haakana P, Nurminen J, Kulmala JP, et al. Effects of cognitive and motor dual-task on gait parameters in children and adolescents with cerebral palsy. Gait & Posture. 2020;81:130-135. [DOI:10.1016/j.gaitpost.2020.07.099]
27. Schmid AB, Dyer L, Böni T, et al. Paraspinal muscle activity during symmetrical and asymmetrical weight training in idiopathic scoliosis. Journal of Sport Rehabilitation. 2010;19(3):315-327. [DOI:10.1123/jsr.19.3.315]
28. Konrad P. The ABC of EMG: a practical introduction to kinesiological electromyography. Scottsdale (AZ): Noraxon Inc.; 2005.
29. Prosser LA, Lee SC, Barbe MF, et al. Trunk and hip muscle activity in early walkers with and without cerebral palsy: a frequency analysis. Journal of Electromyography and Kinesiology. 2010;20(5):851-859. [DOI:10.1016/j.jelekin.2010.04.005]
30. Romkes J, Brunner R. An electromyographic analysis of obligatory and voluntary unilateral toe-walking. Gait & Posture. 2007;26(4):577-586. [DOI:10.1016/j.gaitpost.2006.12.010]
31. Patikas D, Wolf SI, Döderlein L. Electromyographic evaluation of the sound and involved side during gait of spastic hemiplegic children with cerebral palsy. European Journal of Neurology. 2005;12(9):691-699. [DOI:10.1111/j.1468-1331.2005.01047.x]
32. Adjenti SK, Louw G, Jelsma J, Unger M. Electromyographic study of abdominal muscle activity in children with spastic cerebral palsy. South African Journal of Physiotherapy. 2017;73(1):341. [DOI:10.4102/sajp.v73i1.341]
33. Sharifmoradi K, Farahpour N. Range of motion and lower limb muscle activity in Parkinson's disease and elderly individuals. Journal of Sport Biomechanics. 2017;3(1):25-36.
34. Bruijn SM, Millard M, Van Gestel L, et al. Gait stability in children with cerebral palsy. Research in Developmental Disabilities. 2013;34(5):1689-1699. [DOI:10.1016/j.ridd.2013.02.011]
35. Armand S, Decoulon G, Bonnefoy-Mazure A. Gait analysis in children with cerebral palsy. EFORT Open Reviews. 2016;1(12):448-460. [DOI:10.1302/2058-5241.1.000052]
36. Gharib NM, Abd-El Maksoud GM, Eldin S, Elsayed B. Efficacy of concurrent cognitive-motor training on gait in hemiparetic cerebral palsy: a randomized controlled trial. International Journal of Physiotherapy and Research. 2017;5(1):1852-1862. [DOI:10.16965/ijpr.2016.206]
37. Winters TF, Gage JR, Hicks R. Gait patterns in spastic hemiplegia in children and young adults. Journal of Bone and Joint Surgery (American Volume). 1987;69(3):437-441. [DOI:10.2106/00004623-198769030-00016]
38. Ferdjallah M, Harris GF, Smith P, Wertsch JJ. Analysis of postural control synergies during quiet standing in healthy children and children with cerebral palsy. Clinical Biomechanics. 2002;17(3):203-210. [DOI:10.1016/S0268-0033(01)00121-8]
39. Charles J, Gordon AM. A critical review of constraint-induced movement therapy and forced use in children with hemiplegia. Neural Plasticity. 2005;12(2-3):245-261. [DOI:10.1155/NP.2005.245]
40. Zehr EP, Fujita K, Stein RB. Reflexes from the superficial peroneal nerve during walking in stroke subjects. Journal of Neurophysiology. 1998;79(2):848-858. [DOI:10.1152/jn.1998.79.2.848]
41. Kahneman D. Attention and effort. Englewood Cliffs (NJ): Prentice-Hall; 1973.
42. Azadian E, Taheri Torbati H. Muscle activity during dual-task walking in elderly with balance impairments. Journal of Sport Biomechanics. 2016;2(2):5-15.
43. Lima CR, Pavão SL, da Silva BR, et al. Cognitive-motor dual-task costs on postural sway during sit-to-stand movement in children with cerebral palsy. Physiotherapy. 2023;103(4):pzad016. [DOI:10.1093/ptj/pzad016]
44. Piitulainen H, Kulmala JP, Mäenpää H, et al. Gait is less stable in children with cerebral palsy in dual-task conditions. Journal of Biomechanics. 2021;117:110244. [DOI:10.1016/j.jbiomech.2021.110244]
45. Yazdani S, Farahpour N, Delavar A, Farahmand F. Electromyographical activity of erector spinae and gluteus medius muscles in patients with adolescent idiopathic scoliosis during gait. Medical Journal of Tabriz University of Medical Sciences. 2016;38(6):84-92.
46. Hung YC, Meredith GS. Influence of dual-task constraints on gait performance and bimanual coordination during walking in children with unilateral cerebral palsy. Research in Developmental Disabilities. 2014;35(4):755-760. [DOI:10.1016/j.ridd.2014.01.024]
47. Johnson-Frey SH (ed.). Taking action: cognitive neuroscience perspectives on intentional acts. Cambridge (MA): MIT Press; 2003. [DOI:10.7551/mitpress/6614.001.0001]
48. Syczewska M, Święcicka A. Electromyographic patterns during gait in spastic cerebral palsy. Acta of Bioengineering and Biomechanics. 2016;18(3):-.
49. Kulmala JP, Haakana P, Nurminen J, et al. Effort equalization hypothesis in children with cerebral palsy. PLoS One. 2022;17(1):e0262042. [DOI:10.1371/journal.pone.0262042]
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Journal of Sport Biomechanics
Department of Sport Biomechanics, Faculty of Humanities, Islamic Azad University, Hamedan Branch, Prof. Mousivand Blvd, Imam Khomeini Blvd, Hamedan, Iran.
Journal Tel: +98 81 34494042
Website: http://biomechanics.iauh.ac.ir
Email: sportbiomechanics@iauh.ac.ir
