

Volume 12, Issue 3 (11-2026)
J Sport Biomech 2026, 12(3): 406-416 |
Back to browse issues page


![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Bodake P, Welling A, Gurudut P, Kage V. Development of EMG-Guided Exercise Protocol (SCAP-SYNC) for Targeting Scapular Dyskinesia in Swimmers. J Sport Biomech 2026; 12 (3) :406-416
URL: http://biomechanics.iauh.ac.ir/article-1-501-en.html
URL: http://biomechanics.iauh.ac.ir/article-1-501-en.html



1- Department of Orthopaedic Physiotherapy, KAHER Institute of Physiotherapy, Nehru Nagar, Belagavi, Karnataka, India.
2- Department of Orthopedic Physiotherapy, KLE Institute of Physiotherapy, Belagavi, Karnataka, India.
2- Department of Orthopedic Physiotherapy, KLE Institute of Physiotherapy, Belagavi, Karnataka, India.
Full-Text [PDF 1089 kb]
(2 Downloads)
| Abstract (HTML) (8 Views)
Full-Text: (2 Views)
1. Introduction
Scapular dyskinesia (SD) is characterized by abnormal movement or positioning of the scapula during shoulder motion and is commonly observed in competitive swimmers due to the repetitive overhead nature of the sport (1–3). While symptomatic SD receives clinical attention because of its association with pain and dysfunction, asymptomatic SD, in which altered scapular motion occurs without pain, is often underdiagnosed despite its potential to progress to symptomatic injury and negatively affect athletic performance over time (1, 2).
Biomechanically, the scapula serves as a dynamic yet stable base for humeral movement, providing the shoulder girdle with the mobility and stability required for efficient upper-extremity function (1). Swimmers perform thousands of overhead strokes each week, including freestyle, butterfly, and backstroke, placing substantial repetitive demands on the scapulothoracic musculature (4, 5). These repetitive movements may lead to muscle imbalances, fatigue, and dysfunction of the scapular stabilizers, thereby predisposing athletes to SD (1, 6). Epidemiological studies indicate that the prevalence of scapular dyskinesia among swimmers varies considerably, with reported rates ranging from 8.5% to as high as 61% during or immediately after training sessions (3, 7). Asymptomatic SD has been reported frequently in elite young swimmers, with a higher incidence among males and endurance swimmers (3).
Altered scapular kinematics can disrupt normal force transmission throughout the shoulder complex, resulting in reduced stroke efficiency, compromised biomechanics, and an increased risk of secondary pathologies, including shoulder impingement syndrome, rotator cuff tendinopathy, and glenohumeral instability, collectively referred to as “swimmer’s shoulder” (6, 8). Therefore, early identification and intervention are essential to prevent progression from asymptomatic SD to painful dysfunction and performance decline (9).
Conventional screening methods for SD, which often rely on observational or manual assessment techniques, may fail to detect subtle or dynamic muscular imbalances effectively (1, 2). Surface electromyography (EMG) provides an objective and quantitative method for assessing real-time muscle activation patterns during functional activities. This technology enables clinicians and coaches to identify underactive or overactive muscles involved in scapular control more accurately (10, 11), thereby facilitating individualized rehabilitation programs based on neuromuscular function rather than solely on clinical observation (10). Integrating EMG-guided rehabilitation strategies into swimmer conditioning and rehabilitation programs may provide several benefits. In addition to enhancing the strength and endurance of scapular stabilizers, such approaches may improve neuromuscular control and coordination, which are essential for efficient stroke mechanics and injury prevention (4, 9). Improved scapular positioning and movement may facilitate more effective force transfer while minimizing compensatory muscular overload that frequently contributes to overuse injuries in swimmers (5, 11). Furthermore, the incorporation of EMG-guided biofeedback into training may allow rehabilitation strategies to be tailored to the specific neuromuscular deficits of individual athletes, potentially improving rehabilitation outcomes (10).
The importance of early detection and intervention for asymptomatic SD should not be underestimated. Correcting muscular imbalances before the onset of symptoms may help preserve athletic performance and reduce injury-related time loss (2, 9). Moreover, improvements in scapular muscle function and shoulder biomechanics may contribute to enhanced endurance and power production during competitive performance (4, 5). Given these considerations, routine screening of elite swimmers and other overhead athletes using functional assessments supplemented by EMG evaluation should be considered in sports medicine practice (1, 10). Such an approach may facilitate the timely implementation of targeted preventive interventions, with the potential to reduce the incidence of symptomatic shoulder disorders and improve overall shoulder health (8, 9).
Future research should investigate the long-term effectiveness of EMG-guided rehabilitation protocols on performance outcomes, injury incidence, and quality of life. In addition, studies incorporating advanced biomechanical analyses and functional performance measures, such as swimming speed and stroke efficiency, would provide stronger evidence regarding their clinical relevance. Such investigations would further clarify the role of EMG-guided rehabilitation in competitive swimming and may help inform similar protocols for other overhead sports with comparable neuromuscular demands (4, 5, 9). Given the high prevalence of scapular dyskinesia among competitive swimmers and the limitations of conventional rehabilitation approaches, there is a need for evidence-based exercise protocols that specifically target the neuromuscular deficits associated with this condition. Therefore, the purpose of this study was to develop an EMG-guided exercise protocol (SCAP-SYNC) by identifying the scapular stabilization exercises that produce the greatest activation of key scapular stabilizer muscles in swimmers with unilateral asymptomatic scapular dyskinesia.
2. Methods
2.1. Study Design and Participants
This protocol development study was conducted to develop an EMG-guided exercise protocol for swimmers with asymptomatic scapular dyskinesia. Ethical clearance was obtained from the Institutional Ethics Review Committee (Ref. No. 897), and written informed consent was obtained from all participants before enrollment in accordance with the Declaration of Helsinki and institutional ethical guidelines. The study was registered with the Clinical Trials Registry of India (CTRI/2025/01/079223). Eighteen male competitive swimmers aged 19–23 years with clinically diagnosed unilateral asymptomatic scapular dyskinesia were recruited for the study (13). All participants had a minimum of three years of competitive swimming experience and trained 6–7 sessions per week for approximately 1–2 hours per session. The study was conducted at the Advanced Physiotherapy Centre, Gait Laboratory, KLE Hospital, Belagavi, India, between October 2024 and March 2025. Participants were excluded if they had a history of shoulder fracture, shoulder dislocation, whiplash injury, skin hypersensitivity, active skin infection, allergy to conductive gel, or any traumatic or systemic condition that could influence participation or affect study outcomes.
Sample size estimation was performed using G*Power software (Version 3.1, Heinrich Heine University, Düsseldorf, Germany) for a paired-comparison design (paired t-test). Calculations were based on a two-tailed significance level of α = 0.05 and a statistical power of 80% (1−β = 0.80). Based on effect sizes reported in previous studies evaluating scapular stabilizer muscle activation in overhead athletes, the minimum required sample size was estimated at 16 participants. To account for potential dropouts and incomplete EMG recordings, the sample size was increased by approximately 10%, resulting in a final target sample of 18 participants. All recruited participants completed the study.
2.2. Electromyography Setup
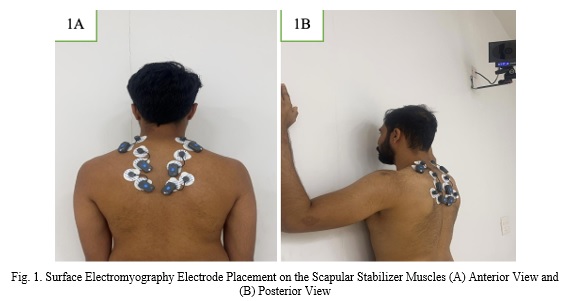
Surface electromyography (EMG) was used to record muscle activity from the primary scapular stabilizer muscles. Electrodes were placed according to SENIAM recommendations over the upper, middle, and lower trapezius, serratus anterior, infraspinatus, rhomboids, and latissimus dorsi muscles bilaterally (Fig. 1A and 1B) (14). Raw EMG signals were recorded while participants performed the prescribed exercise tasks. Muscle activity was assessed on both the affected and unaffected sides to evaluate differences in muscle recruitment patterns associated with unilateral scapular dyskinesia.
Scapular dyskinesia (SD) is characterized by abnormal movement or positioning of the scapula during shoulder motion and is commonly observed in competitive swimmers due to the repetitive overhead nature of the sport (1–3). While symptomatic SD receives clinical attention because of its association with pain and dysfunction, asymptomatic SD, in which altered scapular motion occurs without pain, is often underdiagnosed despite its potential to progress to symptomatic injury and negatively affect athletic performance over time (1, 2).
Biomechanically, the scapula serves as a dynamic yet stable base for humeral movement, providing the shoulder girdle with the mobility and stability required for efficient upper-extremity function (1). Swimmers perform thousands of overhead strokes each week, including freestyle, butterfly, and backstroke, placing substantial repetitive demands on the scapulothoracic musculature (4, 5). These repetitive movements may lead to muscle imbalances, fatigue, and dysfunction of the scapular stabilizers, thereby predisposing athletes to SD (1, 6). Epidemiological studies indicate that the prevalence of scapular dyskinesia among swimmers varies considerably, with reported rates ranging from 8.5% to as high as 61% during or immediately after training sessions (3, 7). Asymptomatic SD has been reported frequently in elite young swimmers, with a higher incidence among males and endurance swimmers (3).
Altered scapular kinematics can disrupt normal force transmission throughout the shoulder complex, resulting in reduced stroke efficiency, compromised biomechanics, and an increased risk of secondary pathologies, including shoulder impingement syndrome, rotator cuff tendinopathy, and glenohumeral instability, collectively referred to as “swimmer’s shoulder” (6, 8). Therefore, early identification and intervention are essential to prevent progression from asymptomatic SD to painful dysfunction and performance decline (9).
Conventional screening methods for SD, which often rely on observational or manual assessment techniques, may fail to detect subtle or dynamic muscular imbalances effectively (1, 2). Surface electromyography (EMG) provides an objective and quantitative method for assessing real-time muscle activation patterns during functional activities. This technology enables clinicians and coaches to identify underactive or overactive muscles involved in scapular control more accurately (10, 11), thereby facilitating individualized rehabilitation programs based on neuromuscular function rather than solely on clinical observation (10). Integrating EMG-guided rehabilitation strategies into swimmer conditioning and rehabilitation programs may provide several benefits. In addition to enhancing the strength and endurance of scapular stabilizers, such approaches may improve neuromuscular control and coordination, which are essential for efficient stroke mechanics and injury prevention (4, 9). Improved scapular positioning and movement may facilitate more effective force transfer while minimizing compensatory muscular overload that frequently contributes to overuse injuries in swimmers (5, 11). Furthermore, the incorporation of EMG-guided biofeedback into training may allow rehabilitation strategies to be tailored to the specific neuromuscular deficits of individual athletes, potentially improving rehabilitation outcomes (10).
The importance of early detection and intervention for asymptomatic SD should not be underestimated. Correcting muscular imbalances before the onset of symptoms may help preserve athletic performance and reduce injury-related time loss (2, 9). Moreover, improvements in scapular muscle function and shoulder biomechanics may contribute to enhanced endurance and power production during competitive performance (4, 5). Given these considerations, routine screening of elite swimmers and other overhead athletes using functional assessments supplemented by EMG evaluation should be considered in sports medicine practice (1, 10). Such an approach may facilitate the timely implementation of targeted preventive interventions, with the potential to reduce the incidence of symptomatic shoulder disorders and improve overall shoulder health (8, 9).
Future research should investigate the long-term effectiveness of EMG-guided rehabilitation protocols on performance outcomes, injury incidence, and quality of life. In addition, studies incorporating advanced biomechanical analyses and functional performance measures, such as swimming speed and stroke efficiency, would provide stronger evidence regarding their clinical relevance. Such investigations would further clarify the role of EMG-guided rehabilitation in competitive swimming and may help inform similar protocols for other overhead sports with comparable neuromuscular demands (4, 5, 9). Given the high prevalence of scapular dyskinesia among competitive swimmers and the limitations of conventional rehabilitation approaches, there is a need for evidence-based exercise protocols that specifically target the neuromuscular deficits associated with this condition. Therefore, the purpose of this study was to develop an EMG-guided exercise protocol (SCAP-SYNC) by identifying the scapular stabilization exercises that produce the greatest activation of key scapular stabilizer muscles in swimmers with unilateral asymptomatic scapular dyskinesia.
2. Methods
2.1. Study Design and Participants
This protocol development study was conducted to develop an EMG-guided exercise protocol for swimmers with asymptomatic scapular dyskinesia. Ethical clearance was obtained from the Institutional Ethics Review Committee (Ref. No. 897), and written informed consent was obtained from all participants before enrollment in accordance with the Declaration of Helsinki and institutional ethical guidelines. The study was registered with the Clinical Trials Registry of India (CTRI/2025/01/079223). Eighteen male competitive swimmers aged 19–23 years with clinically diagnosed unilateral asymptomatic scapular dyskinesia were recruited for the study (13). All participants had a minimum of three years of competitive swimming experience and trained 6–7 sessions per week for approximately 1–2 hours per session. The study was conducted at the Advanced Physiotherapy Centre, Gait Laboratory, KLE Hospital, Belagavi, India, between October 2024 and March 2025. Participants were excluded if they had a history of shoulder fracture, shoulder dislocation, whiplash injury, skin hypersensitivity, active skin infection, allergy to conductive gel, or any traumatic or systemic condition that could influence participation or affect study outcomes.
Sample size estimation was performed using G*Power software (Version 3.1, Heinrich Heine University, Düsseldorf, Germany) for a paired-comparison design (paired t-test). Calculations were based on a two-tailed significance level of α = 0.05 and a statistical power of 80% (1−β = 0.80). Based on effect sizes reported in previous studies evaluating scapular stabilizer muscle activation in overhead athletes, the minimum required sample size was estimated at 16 participants. To account for potential dropouts and incomplete EMG recordings, the sample size was increased by approximately 10%, resulting in a final target sample of 18 participants. All recruited participants completed the study.
2.2. Electromyography Setup
Surface electromyography (EMG) was used to record muscle activity from the primary scapular stabilizer muscles. Electrodes were placed according to SENIAM recommendations over the upper, middle, and lower trapezius, serratus anterior, infraspinatus, rhomboids, and latissimus dorsi muscles bilaterally (Fig. 1A and 1B) (14). Raw EMG signals were recorded while participants performed the prescribed exercise tasks. Muscle activity was assessed on both the affected and unaffected sides to evaluate differences in muscle recruitment patterns associated with unilateral scapular dyskinesia.
2.3. Experimental Procedure
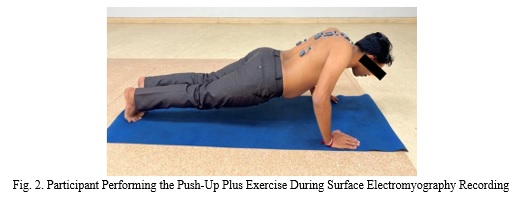
Following screening and informed consent, demographic information was collected and participants underwent baseline assessment. Unilateral scapular dyskinesia was confirmed using the Lateral Scapular Slide Test (LSST) (15). After electrode placement, participants performed 15 commonly prescribed scapular and shoulder stabilization exercises. Each exercise was performed three times, and the highest peak muscle activation value obtained across the three trials was selected for analysis (4). Examples of exercise performance are presented in Fig. 2 and 3. This standardized testing procedure enabled objective assessment of scapular stabilizer activation and provided the basis for identifying exercises that elicited the greatest neuromuscular response.
Following screening and informed consent, demographic information was collected and participants underwent baseline assessment. Unilateral scapular dyskinesia was confirmed using the Lateral Scapular Slide Test (LSST) (15). After electrode placement, participants performed 15 commonly prescribed scapular and shoulder stabilization exercises. Each exercise was performed three times, and the highest peak muscle activation value obtained across the three trials was selected for analysis (4). Examples of exercise performance are presented in Fig. 2 and 3. This standardized testing procedure enabled objective assessment of scapular stabilizer activation and provided the basis for identifying exercises that elicited the greatest neuromuscular response.

2.4. Protocol Development
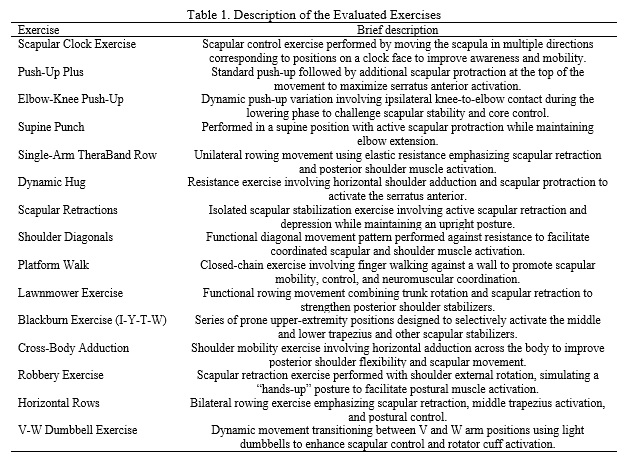
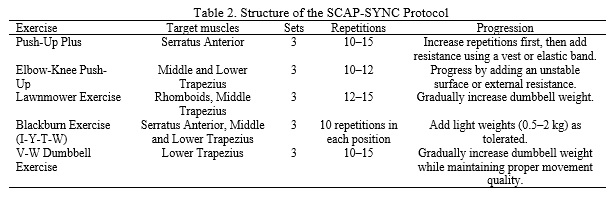
To identify the most effective exercises for scapular stabilization in swimmers with asymptomatic scapular dyskinesia, fifteen commonly prescribed scapular and shoulder stabilization exercises were evaluated using surface electromyography. Muscle activation of the upper, middle, and lower trapezius, serratus anterior, latissimus dorsi, infraspinatus, and rhomboid muscles was recorded during each exercise. EMG data were analyzed to determine which exercises produced the highest activation of the targeted scapular stabilizer muscles. Exercise selection was based on the magnitude of muscle recruitment, statistical significance, and effect size. Five exercises demonstrated superior activation patterns and were therefore selected for inclusion in the SCAP-SYNC (Scapular Synchronization) Protocol. These exercises included the Push-Up Plus, Elbow-Knee Push-Up, Lawnmower Exercise, Blackburn Exercise, and V-W Dumbbell Exercise. The 15 exercises evaluated in the present study are summarized in Table 1.
To identify the most effective exercises for scapular stabilization in swimmers with asymptomatic scapular dyskinesia, fifteen commonly prescribed scapular and shoulder stabilization exercises were evaluated using surface electromyography. Muscle activation of the upper, middle, and lower trapezius, serratus anterior, latissimus dorsi, infraspinatus, and rhomboid muscles was recorded during each exercise. EMG data were analyzed to determine which exercises produced the highest activation of the targeted scapular stabilizer muscles. Exercise selection was based on the magnitude of muscle recruitment, statistical significance, and effect size. Five exercises demonstrated superior activation patterns and were therefore selected for inclusion in the SCAP-SYNC (Scapular Synchronization) Protocol. These exercises included the Push-Up Plus, Elbow-Knee Push-Up, Lawnmower Exercise, Blackburn Exercise, and V-W Dumbbell Exercise. The 15 exercises evaluated in the present study are summarized in Table 1.
Based on the EMG findings, the five exercises demonstrating the highest activation of scapular stabilizers were incorporated into the SCAP-SYNC protocol. The protocol was designed as a progressive neuromuscular training program aimed at improving scapular control, muscular endurance, and shoulder biomechanics in swimmers with scapular dyskinesia. Exercises are recommended three times per week for 6–8 weeks, with progression based on movement quality and exercise tolerance. The SCAP-SYNC protocol has been granted Copyright Registration No. LD-20260186297. The final SCAP-SYNC protocol derived from the EMG analysis is presented in Table 2.
2.5. Outcome Measures
As this was a protocol development study, all outcome measures were assessed during a single baseline evaluation session. No post-intervention assessments were performed because the primary objective was to identify exercises producing the greatest activation of scapular stabilizer muscles for protocol development.
2.6. Lateral Scapular Slide Test (LSST)
The Lateral Scapular Slide Test (LSST) (ICC = 0.95) was used to confirm unilateral scapular dyskinesia. Measurements were obtained bilaterally in three standardized arm positions: (1) arms relaxed at the sides, (2) hands on hips with approximately 45° shoulder abduction, and (3) 90° shoulder abduction with internal rotation. A side-to-side difference greater than 1.5 cm was considered indicative of scapular dyskinesia (15).
2.7. Surface Electromyography
Surface electromyography (ICC = 0.97) was used to assess muscle activation of the upper, middle, and lower trapezius, serratus anterior, latissimus dorsi, infraspinatus, and rhomboid muscles during exercise performance. Bipolar surface electrodes were placed according to SENIAM recommendations, and peak muscle activation values obtained during each exercise were used for analysis and comparison between the affected and unaffected sides.
3. Results
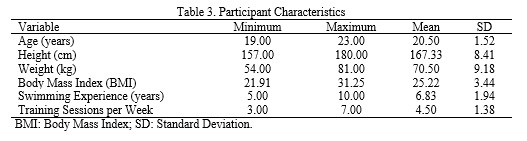
Participant characteristics are presented in Table 3. The recruited swimmers were aged between 19 and 23 years and were all male. Participants had a mean swimming experience of 6.83 ± 1.94 years and participated in an average of 4.50 ± 1.38 training sessions per week. Overall, the sample represented a physically active group of young competitive swimmers. Peak activation of the scapular stabilizer muscles was assessed using surface electromyography (EMG) during the performance of 15 commonly prescribed scapular stabilization exercises. Surface EMG electrodes were placed over the upper, middle, and lower trapezius, serratus anterior, latissimus dorsi, infraspinatus, and rhomboid muscles (Fig 1A and 1B). Mean muscle activation values for each exercise are presented in Table 4.
As this was a protocol development study, all outcome measures were assessed during a single baseline evaluation session. No post-intervention assessments were performed because the primary objective was to identify exercises producing the greatest activation of scapular stabilizer muscles for protocol development.
2.6. Lateral Scapular Slide Test (LSST)
The Lateral Scapular Slide Test (LSST) (ICC = 0.95) was used to confirm unilateral scapular dyskinesia. Measurements were obtained bilaterally in three standardized arm positions: (1) arms relaxed at the sides, (2) hands on hips with approximately 45° shoulder abduction, and (3) 90° shoulder abduction with internal rotation. A side-to-side difference greater than 1.5 cm was considered indicative of scapular dyskinesia (15).
2.7. Surface Electromyography
Surface electromyography (ICC = 0.97) was used to assess muscle activation of the upper, middle, and lower trapezius, serratus anterior, latissimus dorsi, infraspinatus, and rhomboid muscles during exercise performance. Bipolar surface electrodes were placed according to SENIAM recommendations, and peak muscle activation values obtained during each exercise were used for analysis and comparison between the affected and unaffected sides.
3. Results
Participant characteristics are presented in Table 3. The recruited swimmers were aged between 19 and 23 years and were all male. Participants had a mean swimming experience of 6.83 ± 1.94 years and participated in an average of 4.50 ± 1.38 training sessions per week. Overall, the sample represented a physically active group of young competitive swimmers. Peak activation of the scapular stabilizer muscles was assessed using surface electromyography (EMG) during the performance of 15 commonly prescribed scapular stabilization exercises. Surface EMG electrodes were placed over the upper, middle, and lower trapezius, serratus anterior, latissimus dorsi, infraspinatus, and rhomboid muscles (Fig 1A and 1B). Mean muscle activation values for each exercise are presented in Table 4.
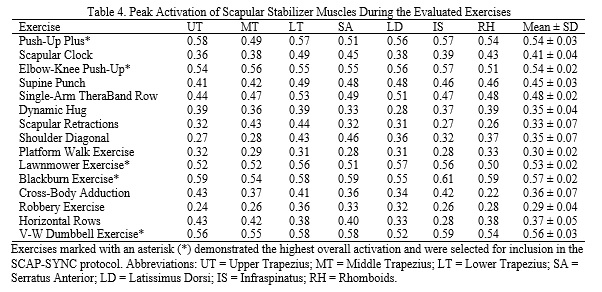
Among the evaluated exercises, the Blackburn Exercise demonstrated the highest overall mean muscle activation (0.57 ± 0.02), followed by the V-W Dumbbell Exercise (0.56 ± 0.03), Push-Up Plus (0.54 ± 0.03), Elbow-Knee Push-Up (0.54 ± 0.02), and Lawnmower Exercise (0.53 ± 0.02). These exercises consistently elicited greater activation of the scapular stabilizer muscles compared with the remaining exercises and were therefore considered the most effective candidates for protocol development.
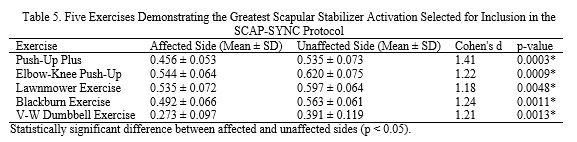
A comparison of peak muscle activation values between the affected and unaffected sides was performed for the five exercises demonstrating the greatest overall muscle activation (Table 5). Significant differences were observed between sides for all five exercises (p < 0.05), with greater activation consistently recorded on the unaffected side.
A comparison of peak muscle activation values between the affected and unaffected sides was performed for the five exercises demonstrating the greatest overall muscle activation (Table 5). Significant differences were observed between sides for all five exercises (p < 0.05), with greater activation consistently recorded on the unaffected side.
The largest effect size was observed for the Push-Up Plus exercise (Cohen’s d = 1.41, p = 0.0003), followed by the Blackburn Exercise (Cohen’s d = 1.24, p = 0.0011), Elbow-Knee Push-Up (Cohen’s d = 1.22, p = 0.0009), V-W Dumbbell Exercise (Cohen’s d = 1.21, p = 0.0013), and Lawnmower Exercise (Cohen’s d = 1.18, p = 0.0048).
These findings indicate substantial differences in scapular stabilizer muscle activation between the affected and unaffected sides and support the selection of these five exercises for inclusion in the SCAP-SYNC protocol. Based on the magnitude of muscle activation, statistical significance, and effect size, the Push-Up Plus, Elbow-Knee Push-Up, Lawnmower Exercise, Blackburn Exercise, and V-W Dumbbell Exercise were selected as the core components of the SCAP-SYNC protocol.
4. Discussion
The purpose of this study was to identify scapular stabilization exercises that elicit high levels of activation in key scapular stabilizer muscles in competitive swimmers with unilateral asymptomatic scapular dyskinesia and to use these findings to develop an EMG-guided exercise protocol. The results demonstrated that five exercises—Push-Up Plus, Elbow-Knee Push-Up, Lawnmower Exercise, Blackburn Exercise, and V-W Dumbbell Exercise—produced the greatest levels of muscle activation and were therefore selected for inclusion in the SCAP-SYNC protocol. Scapular dyskinesia is a common finding in swimmers due to the repetitive overhead demands of training and competition (1–3). Altered scapular motion has been associated with impaired scapulohumeral rhythm, inefficient force transfer, and an increased risk of shoulder pathology (6, 8). Consequently, rehabilitation programs that specifically target the scapular stabilizers are considered important for restoring normal shoulder mechanics and reducing injury risk in overhead athletes (14, 17).
The present findings indicate that exercises combining scapular control, stabilization, and coordinated upper-extremity movement produce greater activation of the scapular stabilizers than several commonly prescribed alternatives. In particular, the Push-Up Plus and Blackburn Exercise demonstrated high overall activation levels, which is consistent with previous studies identifying these exercises as effective strategies for recruiting the serratus anterior and lower trapezius muscles (14, 19). These muscles play a critical role in scapular upward rotation, posterior tilt, and dynamic stabilization during overhead movements. A comparison between affected and unaffected sides revealed significant differences in muscle activation across the selected exercises. Greater activation was consistently observed on the unaffected side, suggesting persistent neuromuscular asymmetry in swimmers with unilateral scapular dyskinesia. Such asymmetries may contribute to altered movement patterns and inefficient load distribution around the shoulder complex, potentially increasing susceptibility to overuse injuries (6, 15).
The SCAP-SYNC protocol was developed by integrating the five exercises that demonstrated the highest activation levels. The protocol combines both closed-chain and open-chain exercises, allowing recruitment of multiple scapular stabilizers through different movement patterns. Closed-chain exercises such as the Push-Up Plus may enhance joint stability and proprioceptive control, whereas open-chain exercises such as the Lawnmower and V-W Dumbbell Exercise may promote coordinated muscle recruitment throughout a greater range of motion (17, 19). An important strength of the present study is the use of surface electromyography to guide exercise selection. Unlike traditional rehabilitation approaches that rely primarily on clinical observation, EMG provides objective information regarding muscle recruitment patterns and allows exercise prescription to be based on quantifiable neuromuscular responses (10, 11). This approach may assist clinicians in selecting exercises that preferentially activate key scapular stabilizers in athletes with scapular dyskinesia. Although the present protocol was developed specifically for competitive swimmers, the underlying principles may also be relevant to other overhead athletes, including volleyball players, tennis players, and baseball pitchers, who similarly depend on efficient scapular control during sport-specific movements (8, 9, 15). However, further investigation is required before the protocol can be generalized to other athletic populations.
Several limitations should be acknowledged. First, the sample size was relatively small (n = 18), which may limit the generalizability of the findings. Second, all participants were male competitive swimmers; therefore, the results may not be directly applicable to female athletes or recreational swimmers. Third, the study focused on acute muscle activation patterns and did not evaluate the long-term effectiveness of the SCAP-SYNC protocol. Future studies should investigate whether implementation of the protocol leads to improvements in scapular function, swimming performance, shoulder symptoms, and injury prevention over time. Longitudinal studies incorporating biomechanical, functional, and clinical outcome measures would provide stronger evidence regarding the effectiveness of the protocol. Overall, the findings suggest that EMG-guided exercise selection may be a useful approach for developing targeted rehabilitation protocols for swimmers with scapular dyskinesia. The SCAP-SYNC protocol provides a structured exercise framework based on objective muscle activation data and may serve as a foundation for future intervention studies.
5. Conclusion
This study developed an EMG-guided exercise protocol (SCAP-SYNC) for swimmers with unilateral asymptomatic scapular dyskinesia by identifying exercises that elicited the highest activation of key scapular stabilizer muscles. Surface EMG was used to objectively determine the exercises that produced the greatest muscle recruitment, resulting in the selection of the Push-Up Plus, Elbow-Knee Push-Up, Lawnmower Exercise, Blackburn Exercise, and V-W Dumbbell Exercise as the core components of the protocol. The findings indicate that swimmers with unilateral scapular dyskinesia exhibit asymmetrical muscle activation patterns, with greater activation observed on the unaffected side. Such asymmetries may contribute to altered scapular control and inefficient load distribution around the shoulder complex. The SCAP-SYNC protocol provides a structured, evidence-based framework for targeting scapular stabilizer muscles in swimmers with scapular dyskinesia. Although the long-term effectiveness of the protocol was not evaluated in the present study, the findings support the use of EMG-guided exercise selection as a rational approach for developing rehabilitation programs. Future intervention studies are warranted to determine whether implementation of the protocol improves scapular function, reduces injury risk, and enhances sport-specific performance outcomes.
Acknowledgment
The authors would like to express their sincere gratitude to Mr. S. B. Javali for his assistance with the statistical analysis. The authors also thank all volunteers who participated in this study and acknowledge the Institute of Physiotherapy, KLE University, Belagavi, for providing the facilities necessary to conduct this research.
Ethical Considerations
Compliance with ethical guidelines
Ethical clearance was obtained from the Institutional Ethics Review Committee (Ref. No. 897). Written informed consent was obtained from all participants prior to participation in the study. The study was conducted in accordance with the principles of the Declaration of Helsinki.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors' contributions
Pradnya Ramling Bodake contributed to the conceptualization and design of the study, methodology development, data collection, data curation, formal analysis, and preparation of the original manuscript draft. Aarti Welling contributed to the conceptualization and methodology of the study, supervised the research process, and critically reviewed and edited the manuscript. Peeyoousha Gurudut contributed to the methodology, validation of the study procedures, supervision of the research activities, and manuscript review and editing. Vijay Kage contributed to supervision, validation, project administration, and critical review and editing of the manuscript. All authors reviewed and approved the final version of the manuscript and agree to be accountable for all aspects of the work.
Conflicts of interest
The authors declare that they have no conflicts of interest.
These findings indicate substantial differences in scapular stabilizer muscle activation between the affected and unaffected sides and support the selection of these five exercises for inclusion in the SCAP-SYNC protocol. Based on the magnitude of muscle activation, statistical significance, and effect size, the Push-Up Plus, Elbow-Knee Push-Up, Lawnmower Exercise, Blackburn Exercise, and V-W Dumbbell Exercise were selected as the core components of the SCAP-SYNC protocol.
4. Discussion
The purpose of this study was to identify scapular stabilization exercises that elicit high levels of activation in key scapular stabilizer muscles in competitive swimmers with unilateral asymptomatic scapular dyskinesia and to use these findings to develop an EMG-guided exercise protocol. The results demonstrated that five exercises—Push-Up Plus, Elbow-Knee Push-Up, Lawnmower Exercise, Blackburn Exercise, and V-W Dumbbell Exercise—produced the greatest levels of muscle activation and were therefore selected for inclusion in the SCAP-SYNC protocol. Scapular dyskinesia is a common finding in swimmers due to the repetitive overhead demands of training and competition (1–3). Altered scapular motion has been associated with impaired scapulohumeral rhythm, inefficient force transfer, and an increased risk of shoulder pathology (6, 8). Consequently, rehabilitation programs that specifically target the scapular stabilizers are considered important for restoring normal shoulder mechanics and reducing injury risk in overhead athletes (14, 17).
The present findings indicate that exercises combining scapular control, stabilization, and coordinated upper-extremity movement produce greater activation of the scapular stabilizers than several commonly prescribed alternatives. In particular, the Push-Up Plus and Blackburn Exercise demonstrated high overall activation levels, which is consistent with previous studies identifying these exercises as effective strategies for recruiting the serratus anterior and lower trapezius muscles (14, 19). These muscles play a critical role in scapular upward rotation, posterior tilt, and dynamic stabilization during overhead movements. A comparison between affected and unaffected sides revealed significant differences in muscle activation across the selected exercises. Greater activation was consistently observed on the unaffected side, suggesting persistent neuromuscular asymmetry in swimmers with unilateral scapular dyskinesia. Such asymmetries may contribute to altered movement patterns and inefficient load distribution around the shoulder complex, potentially increasing susceptibility to overuse injuries (6, 15).
The SCAP-SYNC protocol was developed by integrating the five exercises that demonstrated the highest activation levels. The protocol combines both closed-chain and open-chain exercises, allowing recruitment of multiple scapular stabilizers through different movement patterns. Closed-chain exercises such as the Push-Up Plus may enhance joint stability and proprioceptive control, whereas open-chain exercises such as the Lawnmower and V-W Dumbbell Exercise may promote coordinated muscle recruitment throughout a greater range of motion (17, 19). An important strength of the present study is the use of surface electromyography to guide exercise selection. Unlike traditional rehabilitation approaches that rely primarily on clinical observation, EMG provides objective information regarding muscle recruitment patterns and allows exercise prescription to be based on quantifiable neuromuscular responses (10, 11). This approach may assist clinicians in selecting exercises that preferentially activate key scapular stabilizers in athletes with scapular dyskinesia. Although the present protocol was developed specifically for competitive swimmers, the underlying principles may also be relevant to other overhead athletes, including volleyball players, tennis players, and baseball pitchers, who similarly depend on efficient scapular control during sport-specific movements (8, 9, 15). However, further investigation is required before the protocol can be generalized to other athletic populations.
Several limitations should be acknowledged. First, the sample size was relatively small (n = 18), which may limit the generalizability of the findings. Second, all participants were male competitive swimmers; therefore, the results may not be directly applicable to female athletes or recreational swimmers. Third, the study focused on acute muscle activation patterns and did not evaluate the long-term effectiveness of the SCAP-SYNC protocol. Future studies should investigate whether implementation of the protocol leads to improvements in scapular function, swimming performance, shoulder symptoms, and injury prevention over time. Longitudinal studies incorporating biomechanical, functional, and clinical outcome measures would provide stronger evidence regarding the effectiveness of the protocol. Overall, the findings suggest that EMG-guided exercise selection may be a useful approach for developing targeted rehabilitation protocols for swimmers with scapular dyskinesia. The SCAP-SYNC protocol provides a structured exercise framework based on objective muscle activation data and may serve as a foundation for future intervention studies.
5. Conclusion
This study developed an EMG-guided exercise protocol (SCAP-SYNC) for swimmers with unilateral asymptomatic scapular dyskinesia by identifying exercises that elicited the highest activation of key scapular stabilizer muscles. Surface EMG was used to objectively determine the exercises that produced the greatest muscle recruitment, resulting in the selection of the Push-Up Plus, Elbow-Knee Push-Up, Lawnmower Exercise, Blackburn Exercise, and V-W Dumbbell Exercise as the core components of the protocol. The findings indicate that swimmers with unilateral scapular dyskinesia exhibit asymmetrical muscle activation patterns, with greater activation observed on the unaffected side. Such asymmetries may contribute to altered scapular control and inefficient load distribution around the shoulder complex. The SCAP-SYNC protocol provides a structured, evidence-based framework for targeting scapular stabilizer muscles in swimmers with scapular dyskinesia. Although the long-term effectiveness of the protocol was not evaluated in the present study, the findings support the use of EMG-guided exercise selection as a rational approach for developing rehabilitation programs. Future intervention studies are warranted to determine whether implementation of the protocol improves scapular function, reduces injury risk, and enhances sport-specific performance outcomes.
Acknowledgment
The authors would like to express their sincere gratitude to Mr. S. B. Javali for his assistance with the statistical analysis. The authors also thank all volunteers who participated in this study and acknowledge the Institute of Physiotherapy, KLE University, Belagavi, for providing the facilities necessary to conduct this research.
Ethical Considerations
Compliance with ethical guidelines
Ethical clearance was obtained from the Institutional Ethics Review Committee (Ref. No. 897). Written informed consent was obtained from all participants prior to participation in the study. The study was conducted in accordance with the principles of the Declaration of Helsinki.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors' contributions
Pradnya Ramling Bodake contributed to the conceptualization and design of the study, methodology development, data collection, data curation, formal analysis, and preparation of the original manuscript draft. Aarti Welling contributed to the conceptualization and methodology of the study, supervised the research process, and critically reviewed and edited the manuscript. Peeyoousha Gurudut contributed to the methodology, validation of the study procedures, supervision of the research activities, and manuscript review and editing. Vijay Kage contributed to supervision, validation, project administration, and critical review and editing of the manuscript. All authors reviewed and approved the final version of the manuscript and agree to be accountable for all aspects of the work.
Conflicts of interest
The authors declare that they have no conflicts of interest.
Type of Study: Research |
Subject:
General
Received: 2026/02/10 | Accepted: 2026/05/23 | Published: 2026/06/19
Received: 2026/02/10 | Accepted: 2026/05/23 | Published: 2026/06/19
References
1. Longo UG, Ambrogioni LR, Berton A, Candela V, Massaroni C, Carnevale A, et al. Erratum: Scapular dyskinesis: From basic science to ultimate treatment. International Journal of Environmental Research and Public Health. 2020;17(8):2974. [DOI:10.3390/ijerph17082974]
2. Srinivasan M, Arun Jenikkin A, Shanmugananth Elayaperumal S. Scapular stabilization exercise and tapping for scapular dyskinesia for amateur swimmers: An experimental design. Obstetrics and Gynaecology Forum. 2024;34(2 Suppl):49-52.
3. Maor MB, Ronin T, Kalichman L. Scapular dyskinesis among competitive swimmers. Journal of Bodywork and Movement Therapies. 2017;21(3):633-636. [DOI:10.1016/j.jbmt.2016.11.011]
4. Tavares N, Dias G, Carvalho P, Vilas-Boas JP, Castro MA. Effectiveness of therapeutic exercise in musculoskeletal risk factors related to swimmer's shoulder. European Journal of Investigation in Health, Psychology and Education. 2022;12(6):601-615. [DOI:10.3390/ejihpe12060044]
5. Morais JE, Forte P, Nevill AM, Barbosa TM, Marinho DA. Upper-limb kinematics and kinetics imbalances in the determinants of front-crawl swimming at maximal speed in young international-level swimmers. Scientific Reports. 2020;10(1):11683. [DOI:10.1038/s41598-020-68581-3]
6. Naderifar H, Babakhanian S, Najafi-Vosough R, Ardakani MK. Shoulder function in swimmers with and without scapular dyskinesia. Muscles, Ligaments and Tendons Journal. 2023;13(2):344. [DOI:10.32098/mltj.02.2023.19]
7. Arghadeh R, Alizadeh MH, Minoonejad H, Sheikhhoseini R, Asgari M, Jaitner T. Electromyography of scapular stabilizers in people without scapular dyskinesis during push-ups: A systematic review and meta-analysis. Frontiers in Physiology. 2023;14:1296279. [DOI:10.3389/fphys.2023.1296279]
8. Pesen MF, Vergili Ö. Exploring the relationship between scapular dyskinesia and the injury risk among overhead athletes. Journal of Orthopaedic Research and Rehabilitation. 2023;1(1):1-4. [DOI:10.51271/JORR-0001]
9. Naderifar H, Ghanbari L, Najafi-Vosough R. Effect of an exercise program on glenohumeral rotator cuff muscle strength in overhead athletes with scapular dyskinesia. Journal of Clinical Care and Skills. 2024;5(1):19-24.
10. Du WY, Huang TS, Chiu YC, Mao SJ, Hung LW, Liu MF, et al. Single-session video and electromyography feedback in overhead athletes with scapular dyskinesis and impingement syndrome. Journal of Athletic Training. 2020;55(3):265-273. [DOI:10.4085/1062-6050-490-18]
11. Tsuruike M, Ellenbecker TS, Nishime RS. Electromyographic analysis of the scapular dyskinesis test in a baseball pitcher with a SLAP lesion: A case report. International Journal of Sports Physical Therapy. 2020;15(3):471-479. [DOI:10.26603/ijspt20200471]
12. Zaman BA, Basumatary B, Borah C. Scapular asymmetry among elite swimmers of Jorhat district using lateral scapular slide test. Indian Journal of Physiotherapy and Occupational Therapy. 2021;15(1):1-8.
13. Preziosi Standoli J, Fratalocchi F, Candela V, Preziosi Standoli T, Giannicola G, Bonifazi M, et al. Scapular dyskinesis in young asymptomatic elite swimmers. Orthopaedic Journal of Sports Medicine. 2018;6(1):2325967117750814. [DOI:10.1177/2325967117750814]
14. Kibler WB, Sciascia AD, Uhl TL, Tambay N, Cunningham T. Electromyographic analysis of specific exercises for scapular control in early phases of shoulder rehabilitation. American Journal of Sports Medicine. 2008;36(9):1789-1798. [DOI:10.1177/0363546508316281]
15. Melo AS, Moreira JS, Afreixo V, Moreira-Gonçalves D, Donato H, Cruz EB, et al. Effectiveness of specific scapular therapeutic exercises in patients with shoulder pain: A systematic review with meta-analysis. JSES Reviews, Reports, and Techniques. 2024;4(2):161-174. [DOI:10.1016/j.xrrt.2023.12.006]
16. Curtis T, Roush JR. The lateral scapular slide test: A reliability study of males with and without shoulder pathology. North American Journal of Sports Physical Therapy. 2006;1(3):140-146.
17. Seo SH, Jeon IH, Cho YH, Lee HG, Hwang YT, Jang JH. Surface electromyography during the push-up plus exercise on a stable support or Swiss ball: Scapular stabilizer muscle exercise. Journal of Physical Therapy Science. 2013;25(7):833-837. [DOI:10.1589/jpts.25.833]
18. Kibler WB, Sciascia A. Evaluation and management of scapular dyskinesis in overhead athletes. Current Reviews in Musculoskeletal Medicine. 2019;12(4):515-526. [DOI:10.1007/s12178-019-09591-1]
19. De Mey K, Danneels L, Cagnie B, Cools AM. Scapular muscle rehabilitation exercises in overhead athletes with impingement symptoms: Effect of a 6-week training program on muscle recruitment and functional outcome. American Journal of Sports Medicine. 2012;40(8):1906-1915. [DOI:10.1177/0363546512453297]
20. Wirth K, Keiner M, Fuhrmann S, Nimmerichter A, Haff GG. Strength training in swimming. International Journal of Environmental Research and Public Health. 2022;19(9):5369. [DOI:10.3390/ijerph19095369]
21. Sadri SF, Saleki M. The effect of a combined scapular and shoulder exercise program with kinesio tape on pain, shoulder proprioception, and upper limb function in swimmers with shoulder impingement syndrome. Journal of Sport Biomechanics. 2024;10(2):144-158. [DOI:10.61186/JSportBiomech.10.2.144]
22. Darchini M, Darzabi T, Mofrad Moghadam M, Nabavinik M. The effect of a 6-week core stability training program on the stroke index and front crawl record of male swimmers. Journal of Sport Biomechanics. 2019;5(2):124-133. [DOI:10.32598/biomechanics.5.2.6]
23. Harati J, Daneshmandi H, Shahabi Kaseb MR. Comparing the effects of dry-land and in-water core stability training programs on swimmers' upper body balance and performance. Journal of Sport Biomechanics. 2018;4(1):17-29.
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Journal of Sport Biomechanics
Department of Sport Biomechanics, Faculty of Humanities, Islamic Azad University, Hamedan Branch, Prof. Mousivand Blvd, Imam Khomeini Blvd, Hamedan, Iran.
Journal Tel: +98 81 34494042
Website: http://biomechanics.iauh.ac.ir
Email: sportbiomechanics@iauh.ac.ir
